Advances in Animal and Veterinary Sciences
Research Article

Diagnosis of Granulosa Cell Tumors in Arabian Mares by Ultrasonography, Hormonal Profile and Histopathology
Reda M. S. Korany1*, M. K. Derbala2, T. E. Mosallam2, M. Fadel2, A. H. Aly2, M. E. Essmail2
1Department of Pathology, Faculty of Veterinary Medicine, Cairo University, Giza, 12211, Egypt; 2Animal Reproduction Research Institute, ARC, Giza, 12556, Egypt.
Abstract | Granulosa cell tumors (GCTs) found to be the most common ovarian tumor in mares. This work was aimed to assess the GCT by different investigatory methods as, ultrasonography, hormonal profile and histopathology. 62 Arabian mares aged between 4- 15 years were admitted to hospital with various behavioral changes, these mares examined physically, ultrasonographicaly and by assessment of hormonal profile, ovariectomy was indicated, gross and histopathological evaluation of removed ovaries was performed. Ultrasonographic scanning encountered different types of GCT, that appeared as honeycomb appearance, cystic, solid mass and mixed pattern. The hormonal profile showed higher levels of AMH, progesterone, estrogen and testosterone compared with control group. Histopathologic investigation ensured the presence of GCT in all examined cases with different tumor patterns, although the tumor in all cases was benign. In conclusion, GCT in mares can be diagnosed by ultrasonography, hormonal assays and histopathology. Most cases of GCTs are benign and most affected side is left one. The treatment of choice in case of GCTs is ovariectomy.
Keywords | GCTs, Arabian mares, Ultrasonography, Hormonal profile, Histopathology
Received | December 14, 2019; Accepted | February 17, 2020; Published | March 05, 2020
*Correspondence | Reda M. S. Korany, Department of Pathology, Faculty of Veterinary Medicine, Cairo University, Giza, 12211, Egypt; Email: reda.pathology@yahoo.com, mohamed_equine@yahoo.com
Citation | Korany RMS, Derbala MK, Mosallam TE, Fadel M, Aly AH, Essmail ME (2020). Diagnosis of granulosa cell tumors in arabian mares by ultrasonography, hormonal profile and histopathology. Adv. Anim. Vet. Sci. 8(3): 327-332.
DOI | http://dx.doi.org/10.17582/journal.aavs/2020/8.3.327.332
ISSN (Online) | 2307-8316; ISSN (Print) | 2309-3331
Copyright © 2020 Korany et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
INTRODUCTION
Granulosa cell tumor (GCT) represents the most common ovarian tumor in cow and mare. It is classified as sex-cord stromal tumor. It consists of irregular accumulation of granulosa cells separated by a supporting stroma, imparting a distinct resemblance to follicle formation. They are usually benign, however in queens, bitches and cows they are considered more malignant than in mares (Švara et al., 2009).
Granulosa cell tumor (GCT) is a relatively common cause of ovarian pathology in mares (Kummer et al., 2010).
Prolonged anestrus, aggressive or stallion-like behaviour, and persistent estrus and nymphomania are behavioral disorders which may be observed in mares with GCT (Troedsson et al., 2003).
Most affected mares have been reported to have unilateral affection and clinically appeared with some behavioural changes, it is suggested that a diagnosis can be performed by identifying unilateral ovarian enlargement, with atrophy of the contralateral ovary. However, the presence of active contralateral ovary has been found (Sherlock et al., 2016).
Granulosa cell tumor are often unilateral, slow growing, and benign. Diagnosis of it through transrectal ultrasonography shows a multicystic or honeycombed structure but GCT may also be found as a solid mass or single large cystic cavitation. The contralateral ovary is often small and inactive although some mares with unilateral GCT have a functional contralateral ovary (McCue, 1992).
As the tumor is hormonally active, hormonal disturbances may be reported, including high serum testosterone level. Recently, anti- Meullerian hormone has been recorded to be a diagnostic parameter for GCT (Crabtree et al., 2013). However, some mares may have normal ovarian activity on the other ovary, so final diagnosis of GCTs is confirmed by histopathological evaluation (Maurice, 2005).
Histopathological distinction between different types of ovarian tumors is clear in most cases (Švara et al., 2009).
The commonly used therapy for GCT is surgical interference, ovariectomy is used to remove the tumor, consequently recovers the fertility, so it is important to differentiate between GCT and other causes of ovarian enlargement (Sherlock et al., 2016).
Aim of work
This study was aimed to evaluate the ovarian GCT in Arabian mares on the bases of ultrasonographic, hormonal and histopathological findings.
MATERIALS AND METHODS
Animals
62 Arabian mares aged between 4- 15 years were admitted to Derbala equine clinic with either history of stallion like-behavior, prolonged anestrous, maiden mares had a well-developed clitoris and one case of them had a history of abortion.
Ultrasound examination
Ultrasonography was performed using 2 real time B-mode ultrasound scanners, (Sonoscape-China) equipped with 4-7.5 MHz frequency linear-array rectal transducer and (Esaote Mylab30-Ntherlands) equipped with 5-7.5 MHz frequency linear-array rectal transducer. The scanner has a built-in electronic caliper system for measuring distance, area and circumference, angle and auto follow measurements. Ultrasonic gel (Carboxymethyl cellulose) was used as a lubricant during scanning. Ultrasonographic scan was performed once every week for 3 successive scans for evaluation of GCT and recording any cyclic changes.
Blood sampling
Blood samples were collected from jugular vein before surgery in sterile centrifuge tubes and left to clot and centrifuged at 3000 rpm for 15 minutes to separate sera. Sera aliquots were stored at -20˚C for further detection of hormonal profile.
Hormonal assay
Determination of serum anti-mullerian hormone (AMH), progesterone (P4), estrogen and testosterone concentrations were performed using minividas (automated immunoanalyzer), BioMerivex, France. All the assay steps were performed automatically by the instrument. The intensity of florescent product was measured at 450 nm (Anckaert et al., 2002).
Anesthesia and surgery
General anesthesia was performed for ovarectomy using total intravenous anesthesia (TIVA). The induction was carried out using I/V xylazine (1.1 mg/kg) followed by ketamine (2.2 mg/kg I/V), then maintaining anesthesia through Triple Drip (1 g ketamine and 500 mg xylazine added to 10% guiaphenesin), according to Hall et al., 2001.
Ovarectomy was performed through flank laparotomy approach in lateral recumbency (Loesch and Rodgerson, 2003). Aspiration of large cystic structure in the ovary helps to reduce the size of a big ovary to facilitate exteriorization. TA-90 stapler was used for control the bleeding and ligation of ovarian stump (Trotter and Embertson, 1999).
Histopathological examination
Collected ovaries from surgery were fixed in 10% neutral buffered formalin and routinely processed. The paraffin embedded blocks were sectioned at 5 micron thickness and stained with Hematoxylin and Eosin (Bancroft et al., 2012) for histopathological examination by a light microscope (Olympus BX50, Japan).
Statistical analysis
All results were expressed as mean ± SEM. Statistical analyses were performed using the SPSS version 24.0 statistical analysis package (SPSS, Inc., Chicago, IL, USA). The parametric test one-way ANOVA was used for data analysis and comparison was done using Turkey post-hoc test. In all calculations, a difference at P < 0.05 was considered significant.
RESULTS
Physical examination
On physical examination, the total number of mares that exhibited granulosa cell tumor (GCT) was 62 (15 maiden and 47 multiparous mares). Through physical examination of the vulva, 10 maiden mares showed well developed clitoris (10/15) (Figure 1a and b).
Ultrasonographic findings
By trans-rectal sonographic examination of the affected mares, the highest incidence of GCT in this study was observed in the left ovary and the lowest incidence was in the right one (40/62 for left ovary and 22/62 for the right ovary; 64.5% and 35.5% respectively). With ultrasonography scanning, GCT showed enlarged ovary that characterized either by one cystic or double cystic structure, honeycomb appearance, solid structure or mixed honeycomb and cystic structure as shown in the Table 1 and Figure 2a, b, c and d.
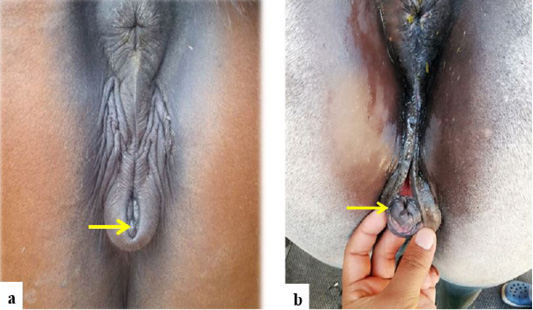
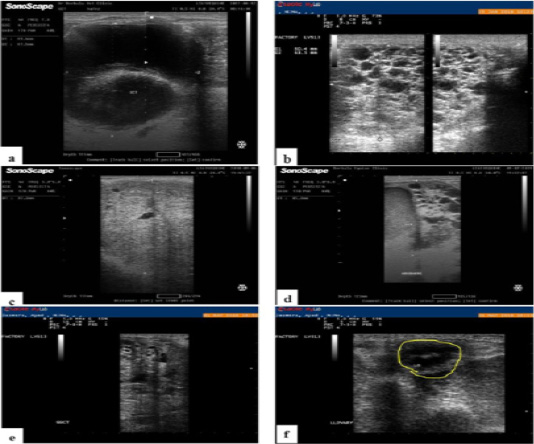
Figure 2: a, Ultrasound image of Arabian mare ovary with granulosa cell tumor showing double large cystic dilatations. b, Ultrasonographic image of Arabian mare ovary with GCT showing multiple cysts with typical honeycomb appearance. c, Ultrasound image of ovary of Arabian mare with granulosa cell tumor. Note the solid mass with few very small cystic cavitations. d, Ultrasound image of Arabian mare ovary with granulosa cell tumor. Note presence of mixed pattern of the tumor. e, ultrasonography showing right ovary with GCT and f, atrophied and non-functioning left ovary of the same case.
Table 1: The incidence of different types of GCT in all examined cases.
| Honeycomb |
Cystic or double cystic |
Solid | Mixed | Total | |
| Number | 32 | 10 | 5 | 15 | 62 |
| Percentage | 51.61% | 16.13 | 8.06% | 24.2% | 100% |
With frequent examination with ultrasound there were no changes in the echotexture of the affected ovary with GCT and the contralateral ovary became smaller in size and atrophied (Figure 2e and f).
Hormonal profile
Hormonal profile of control mares and mares with GCT was illustrated in Table 2. Serum concentration of anti-mullerian hormone (AMH), progesterone (P4), estrogen and testosterone showed significant elevation in mares with GCT when compared with control mares (p≤0.05).
Table 2: Hormonal profile of control mares and mares with GCT.
|
AMH (ng/ml) |
P4 (ng/ml) |
Estrogen (pg/ml) |
Testosterone (pg/ml) |
|
| Control |
1.37±0.09a |
1.25±0.29a |
141.33±22.18a |
0.19± 0.043a |
| GCT |
4.46±0.57b |
2.31±0.63b |
187±20.98b |
0.59±0.057b |
Data was expressed as mean ± SEM. b Significantly different from control mares at (p≤0.05).
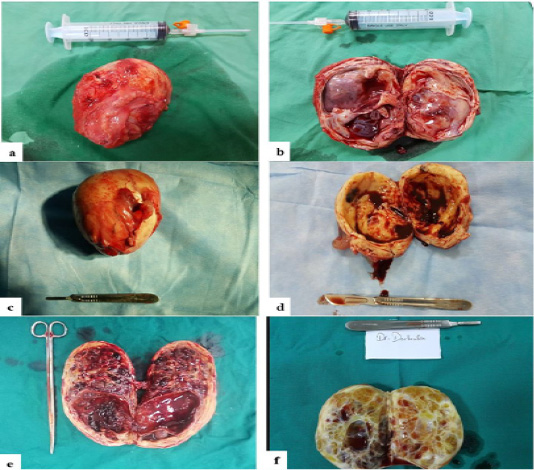
Figure 3: a, Gross appearance of surgically removed ovary of Arabian mare with granulosa cell tumor showing enlarged ovary. b, On section of the same ovary, the tumor reveals multiple large cysts with atrophied ovarian tissue. c, Arabian mare ovary with granulosa cell tumor showing ovary with increased size. d, On section, the tumor has a central large cavity filled with hemorrhagic fluid that exerts pressure atrophy on ovary. e, incised ovary of Arabian mare showing mixed type of granulosa cell tumor, the tumor reveals a large cystic cavity and multiple small cysts. f, a section of Arabian mare ovary. Note the thickened ovarian wall with multiple irregular small cystic spaces (honey comb- like appearance).
Gross pathology
After surgical removal of ovaries with granulosa cell tumor, ovaries were evaluated grossly. The tumors were unilateral and the affected ovary was mostly the left one, the tumors were benign in all cases. Sizes of these tumors was 5x5 cm or larger in some cases, and their weight had very wide range, it ranged from 250 gm. to 4.5 kg. Ovaries showed different pattern of gross appearance. Some cases showed multiple large cystic cavitations with atrophied ovarian tissue (Figure 3a and b). Some ovaries revealed central large cystic cavitation filled with hemorrhagic fluid and exerted pressure atrophy on surrounding ovarian tissue (Figure 3c and d). Some incised ovaries showed a large cystic cavity with multiple small cysts (Figure 3e). Some cases exhibited multiple irregular small cystic spaces scattered all over the ovarian tissue with typical honey comb- like appearance (Figure 3f), and in some cases ovaries appeared as a solid mass with a few very small cavities.
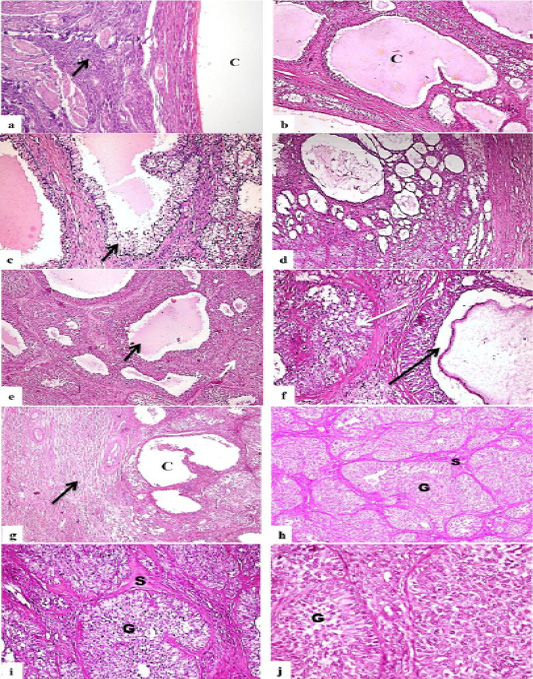
Figure 4: Photomicrograph, ovaries of Arabian mares with GCT. a, ovary showing single large cyst lined with granulosa cells (C), note remaining inactive ovarian tissue (arrow) (H and EX200). b, ovary showing variably-sized cysts (C) that lined with granulosa cells and their lumen filled with homogenous esinophilic structure (HandEX200). c, ovay with GCT, note the multiple large cavities that lined with granulosa cells (arrow) and filled with homogenous esinophilic structure (H and EX200). d, ovary showing multiple and variably-sized cystic cavitation in form of honey-comb like pattern (H and EX100). e, ovary showing a mixed pattern of follicular (black arrow) and solid mass (white arrow) GCT (H and EX200). f, higher magnification of the previous photo showing the follicular-like pattern (black arrow) and solid pattern (white arrow) (H and EX400). g, ovary with mixed solid and cystic GCT (C) showing inactive ovarian tissue surrounding focal tumor mass (arrow) (H and EX100). h, ovary showing solid granulosa cells tumor, tumor cells tend to be arranged in a group of cells (G), each group of cells was separated by connective tissue stroma (S) (H and EX100). I, solid GCT showing groups of granulosa cells (G) surrounded by fine connective tissue stroma (S) (H and EX200). j, higher magnification of the previous photo showing large, vacuolated granulosa cells with prominent nuclei (G) (H and EX400).
Histopathological findings
Histopathological examination of ovaries with GCT showed a great variety in the pattern of the tumor. Some cases revealed presence of one large cystic dilation lined with granulosa cells and surrounded by inactive ovarian tissue (Figure 4a). Other cases showed numerous variably-sized cystic cavitations that lined with granulosa cells and their lumen filled with homogenous esinophilic structure (Figure 4b). Some examined sections appeared with multiple large cavities that lined with granulosa cells and filled with homogenous esinophilic structure, granulosa cells were polyhedral, with defined margins and scanty amounts of eosinophilic cytoplasm; nuclei were rounded (Figure 4c). Some tumors appeared microscopically as multiple and variably-sized cystic cavitation that gave the honey-comb like structure (Figure 4d). There were cases showed a mixed pattern of follicular and solid mass GCT in which the granulosa cells appeared to line a follicular-like structure in a pattern similar to the normal ovarian follicles and other granulosa cells appeared to be arranged in a compact manner (Figure 4e, f and g). Tumor in other cases tended to be arranged in a solid mass, as granulosa cells appeared to be arranged in a group of cells, each group of cells was separated by connective tissue stroma, granulosla cells were large with defined margins and faint eosinophilic cytoplasm; nuclei were rounded (Figure 4h, i and j).
DISCUSSION
Ovarian tumors are common in all domestic animals (Švara et al., 2009). GCT found to be the most common ovarian tumor in mares that represents about 2.5–6% of all equine tumors (Crabtree et al., 2013). In this study, mares with GCT aged between 4- 15 years old were presented with a history of stallion like- behavior, prolonged anestrous, maiden mares had a well-developed clitoris and this result was discussed previously by Packer and McKane, 2012. Most of the mares affected with GCT are middle-aged; however, GCT has been reported in mares of all ages, including neonates, older foals and yearlings (Sherlock et al., 2016). Granulosa cell tumor more commonly occurs in middle-aged mares or older and have been rarely reported in mares younger than 4 years old. There is no characteristic clinical manifestation for GTCT, and a variety of clinical signs may be present, depending on the severity of the disease (Patrick et al., 2003). Mares with GTC tumors usually present with behavioral abnormalities, abdominal discomfort and irregular estrus cycle (Packer and McKane, 2012). Mares affected with GTCT often exhibit irregular estrous cycles characterized by either anestrus or nymphomania; stallion-like behavior or aggressiveness is common (Frederico et al., 2007). Production of hormones in ovary affected with GCT may result in various behavioural changes and alterations in estrus cycle (Švara et al., 2009).
Trans-rectal sonographic examination of the affected mares in this study showed that, the highest incidence of GCT was observed in the left ovary and the lowest incidence was in the right one. With ultrasonography scanning, GCT showed enlarged ovary that characterized either by one cystic or double cystic structure, honeycomb appearance, solid structure or mixed honeycomb and cystic structure. The contralateral ovary became smaller in size and atrophied and this result came in agreement with Sherlock et al., 2016. Trans-rectal ultrasound appearance of GCTs varies, but they most commonly have the appearance of multilocular (‘honeycomb’) masses (Sherlock et al., 2016). Transrectal palpation and ultrasonography reveal an abnormally enlarged ovary accompanied by an inactive contralateral one. Ultrasonographic examination of GCT typically shows the presence of multicystic compartments, resulting in the so-called honey comb appearance. A single large central cyst containing hypoechoic fluid may be observed (Frederico et al., 2007).
In this study, serum concentration of anti-mullerian hormone (AMH), progesterone (P4), estrogen and testosterone showed significant elevation in mares with GCT when compared with control mares and this elevation interpreted the apparent abnormal sexual behavior appeared on examined mares. Hormonal disturbances assessed in this study were agreed with that found by Frederico et al., 2007. Serum hormone levels are a useful diagnostic approach for GCT. Serum testosterone values can be used to diagnose GCTs, as the plasma testosterone levels are elevated in approximately 50% of mares with this tumor (Maurice, 2005). The abnormal reproductive behavior observed in mares with GCTs has been attributed to the influence of steroid hormones secreted from hormonally active tumors. Types and amounts of hormones secreted by individual tumors vary considerably. Aggressive and stallion-like behavior has been associated with high circulating levels of testosterone; however, it has also been observed that testosterone secretion may be episodic (Sherlock et al., 2016). Granulosa cell tumors may produce different combinations of testosterone, inhibin, and estrogen. Behavioral changes vary from stallion-like to nymphomania, and even anestrus. These patterns of behavior may be associated with the predominant hormone secreted by the GCT. Excessive hormone production by a GCT also affects the reproductive capability of a mare due to an inhibitory influence on the unaffected ovary (Frederico et al., 2007). GCTs are the most common ovarian tumors in mares and result in increased plasma concentrations of hormones as testosterone, estrogen, progesterone, and inhibin. These cause a variety of reproductive and behavioral changes, including anestrus, constant or erratic estrus, or stallion-like behaviors (Maurice, 2005). AMH was detected in granulosa cells of small antral follicles and was decreased in larger follicles from normal ovaries. These data indicate that AMH is useful biomarker for GCT and normal follicular development in mares (Ball et al., 2008).
In this study, surgical removal of ovaries (ovariectomy) of all cases was the treatment of choice according to that recommended by Maurice, 2005. GCT is the most common ovarian tumor found in mare and the most frequent indication for non-elective ovariectomy (Frederico et al., 2007). Due to the various reproductive and behavioral abnormalities in mares with GCTs, surgical removal of the affected ovary is the treatment of choice (Maurice, 2005).
After ovariectomy, ovaries of all cases evaluated grossly and the gross picture was compatible with that obtained by ultrasonography that used for primary diagnosis of GCT.
Histopathological examination of ovaries showed a great variety in the pattern of the tumor. Some cases revealed presence of large cystic dilation lined with granulosa cells and surrounded by inactive ovarian tissue. Other cases showed numerous variably-sized cystic cavitations that lined with granulosa cells and their lumen filled with homogenous esinophilic structure. Some appeared with multiple large cavities that lined with granulosa cells and filled with homogenous esinophilic structure. Some tumors appeared microscopically as multiple and variably-sized cystic cavitation that gave the honey-comb like structure. There were cases showed a mixed pattern of follicular and solid mass GCT in which the granulosa cells appeared to line a follicular-like structure in a pattern similar to the normal ovarian follicles and other granulosa cells appeared to be arranged in a compact manner. Tumor in other cases tended to be arranged in a solid mass. GCT in all examined cases was benign according to histopathological finding, so the histopathological examination of the tumor was a helpful tool with the other diagnostic tools to assess the pattern of tumor growth and the behavior of tumor either benign or malignant. Granulosa cell tumor is usually benign (Švara et al., 2009). History, clinical signs, trans-rectal palpation, ultrasonography and hormonal assays are useful in diagnosis of GCTs. As testosterone, progesterone, and estrogen are normally produced by ovarian tissue, so the interpretation of their values can be difficult in cases of GCTs. Also, some mares with GCTs may continue to have normal ovarian activity on the other ovary, so the final diagnosis is obtained by histopathological examination of ovarian tissue (Maurice, 2005). When mares represented with stallion-like behavior, GCT was considered most likely. Histological diagnosis of GCT is usually straightforward, although there are different patterns of tumor (Crabtree et al., 2013). So, ultrasonography, hormonal Profile and histopathology should be performed altogether to reach and confirm the final diagnosis of GCT.
CONCLUSION
From this study we concluded that, GCT in mares can be diagnosed on bases of History, clinical signs, ultrasonography, hormonal assays and histopathology, moreover most of GCTs are benign and most affected side is left side, and finally the treatment of choice in these cases was surgical removal of the ovaries.
Authors’ Contributions
All authors contributed equally in the planning of the study, drafting the manuscript. All of them approve the final version of the article.
Ethical animal research
Ethical approval not required.
Conflict of interest
The authors declare that they have no conflict of interests.
REFERENCES



