Journal of Infection and Molecular Biology
Review Article
Journal of Infection and Molecular Biology 1 (2): 27 – 31Bedside Diagnosis of Common Flu and Flu–Dependent Brain X Syndrome
Sergi Stagnaro1*, Simone Caramel2
- Erasmo Piaggio N 23/8 – 16039 Riva Trigoso, Genova – Honorary President of International Society of Quantum Biophysical Semiotics (SISBQ), Italy
- Doberdò, 3 – 31020 Fontane di Villorba, Treviso – President of International Society of Quantum Biophysical Semiotics (SISBQ) – CP 18 – 31020 Lancenigo – Italy
*Corresponding author:simonecaramel@yahoo.it
ARTICLE CITATION:
Stagnaro S, Caramel S (2013). Bedside Diagnosis of Common Flu and ‘Flu–Dependent Brain X Syndrome. J. Inf. Mol. Biol. 1 (2): 27 – 31.
Received: 2013–04–09, Revised: 2013–06–08, Accepted: 2013–06–24
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/2/44/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
From clinical perspective, it is imperative to diagnose different types of flue including A/H1/N1. To accomplish this, we introduced the Quantum Biophysical Semeiotics (QBS) theory and its clinical methodology and applications. QBS method allows the clinical and pre–clinical diagnosis of the most severe diseases, including cancer, both solid and liquid, coronary heart diseases, as well as Type 2 Diabetes Mellitus, i.e., through the auscultatory percussion of the stomach. General Practitioners can now evaluate, with a stethoscope and the auscultation of any viscera (i.e. stomach, spleen, ureters), mitochondria functions, as well as the behaviour of any biological system, for diagnostic purposes of infections, including flu.
INTRODUCTION
In this paper we illustrate the bedside QBS diagnosis of the various types of flu, including A/H1N1, in spite of the sophisticated semeiotics (who’s specificity/sensitivity is about 60%), certainly not applicable on large scale diagnosis. In addition, all antiviral drugs must be utilized in the first stage of disorder. As a matter of facts, nowadays it is very difficult to know the real nature of an infectious disorder both at the bed–side and Emergency Room (ER) or hospital, as well as to recognize the vast majority of cases, not to speak of other disorders recognizable by means of the physical semeiotics (Jernigan et al., 2009; Kawachi et al., 2009; Bellmann–Weiler et al., 2011).
In fact, the majority of general practitioners around the world agree with the uncertainty of the value of antibiotics for acute tonsillitis, pharyngitis, bronchitis in the form of written and verbal advice, often without physical examination (Chertow et al., 2013). Flu diagnosis is often very difficult to be made from the clinical and laboratory view–point, in particular if clinical phenomenology is misleading, as it happens frequently: vertigo, lipothymia, nausea, vomiting, with or without diarrea, precordialgia, and so on (Hauge et al., 2009; Yasuda et al., 2012; Jacobus et al., 2012; Talbot et al., 2010; Hatchette et al., 2009; Moreno et al., 2011). In addition, in single patient, pre–existing pathological conditions, e.g., recent subarachnoidal or intra–parenchymal cerebral hemorrhage surgical intervention, could confuse diagnostic procedure at the bed–side (personal experience) (Stagnaro et al., 2004b).
By means of QBS theory and method, physicians are able to recognize easily and quickly the “chronic” antibodies synthesis, but not the acute one, i.e., in the spleen during flu, which is a typical early and acute sign of viral infection. Interestingly, the spleen “small” antibody production is a characteristic of Gram–negative bacterial infection.
From the above information, one understands the central diagnostic role played by spleen antibody production in bed–side differential diagnosis between flu virus or Gram–negative infections (Stagnaro et al., 2004a). Moreover, physicians can now–a–day observe clinically, and in a “quantitative” way, the so–called Reticulo–Endothelial–System–Hyperfunction Syndrome (RESH), that is more reliable than the ‘Erythrocyte Sedimentation Rate’ (ESR) (Stagnaro, 1983a). Finally, we introduce, for the first time, a new syndrome termed ‘Flu–dependent Brain X Syndrome’.
BEDSIDE DIAGNOSIS OF FLU: QBS SIGNS
According to QBS theory, flu can be diagnosed in several ways, as described earlier (Stagnaro et al., 2004a; Stagnaro, 2009b; Stagnaro, 2009c). Among different QBS signs, we present the easier and exhaustive method in daily practice for flu diagnosis, taking into account the Tissue Microvascular Unit (TMU), in particular through the clinical auscultatory percussion of finger pulp.
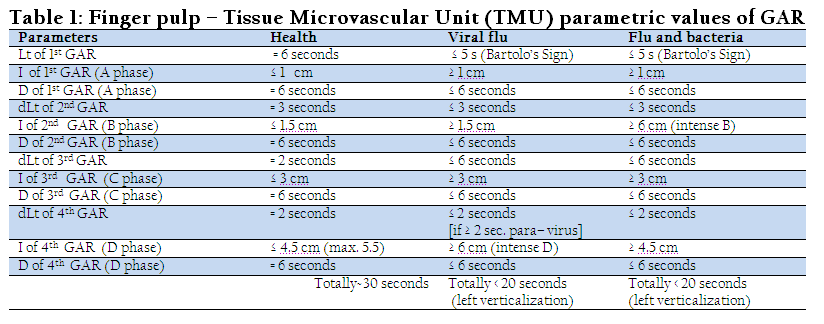
The background information of ‘Auscultatory Percussion of the Stomach’ (APoS), has been presented earlier (Stagnaro et al., 2004a; 2004b). Simply, the APoS allows to recognise the ‘Gastric Aspecific Reflex’ (GAR) and the ‘tonic Gastric Contraction’ (tGC), and to assess the main informative parameters of these reflexes: the ‘Latency time’ (Lt), in seconds, the duration (D), in seconds, the intensity (I), in cm, the reflex disappearing time or ‘differential Latency time’ (dLt), i.e., the pause, in seconds, between two reflexes, as well as the ‘Microcirculatory Functional Reserve’ (MFR) and the ‘fractal Dimension’ (fD) revealed by the above mentioned informative values.
In healthy persons, during their second and third decade of life, under a light–moderate digital pressure on the finger pulp, we observe the following reflex parameters, as summarised in Table 1 (second column). To distinguish between flu and para–flu, we need to look at the different speed of the 4th re–enforcement: if it appears quickly (less than 2 seconds) there is a flu virus, otherwise (more than 2 seconds) this is a sign of para–flu viruses. In other words, bed–side differential diagnosis between flu– and para–flu infection is possible and rapid, because it depends on the necessary time for the occurrence of the 4th re–enforcement.
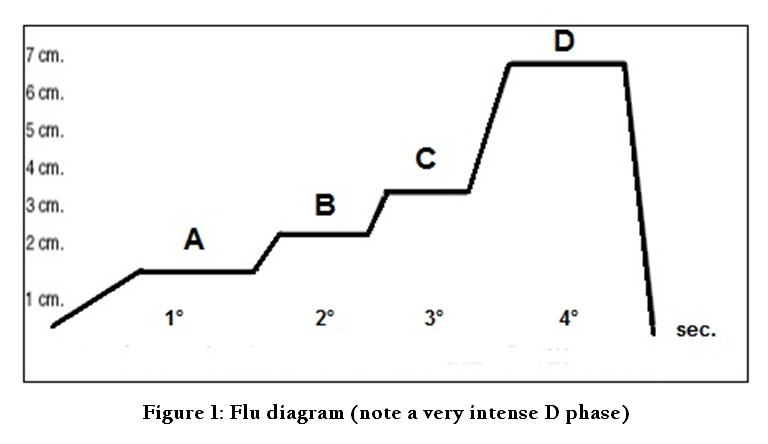
We can define QBS diagrams as geometrical designs of the parametric values of GAR resumed in Table 1, and its subsequent enhancements, brought about by digital pressure upon TMU of finger–pulp, femoral vein at groin, superficial lymphatic vessels, e.g., at the level of internal surface of arm, and finally of an artery, e.g., brachial artery.
Physicians carry out a diagram by trans–locating these parameters values on a Cartesian axes system (Figure 1). The intensity (I) of GAR, in cm, is evidenced on the ordinate (Y) axes, while the ‘Latency time’ (Lt) of GAR as well as its re–enforcements and their duration (D), in seconds, are reported in the abscissa (X) axes. Figure 1 shows the GAR behaviour during digital “mean–intense” pressure applied on a finger–pulp of an individual lying down in supine position, involved by flu: Lt of 1st reflex is shorter than the physiological one: positive Bartolo’s sign (Lt is 4–5 seconds instead of 6 seconds in physiological condition); the 4th reflex appears very intense, indicating characteristically a flu episode, starting from initial symptomless stage. Figure 1 does not show the tonic Gastric Contraction (tGC) after the end of phase 4, followed by a final, small GAR (Z wave), caused by interruption of the pressure on finger–pulp, i.e., the stomach return to its initial size in 2–3 seconds revealing the Oxygen Recovery Time (ORT). On the contrary, always in case of positive Bartolo’s sign, an intense B phase reveals a bacteria’s infection. Summarizing, the most informative parameters are an intense D phase in case of flu and an intense B phase in presence of bacteria.
THE ‘RETHICULO–ENDOTHELIAL–SYSTEM–HYPERFUNCTION’ SYNDROME
The diagram of finger–pulp TMU (Figure 1) is reliable for a correct flu diagnosis. Other numerous QBS signs, sensitive and specific, allow physicians to definitively diagnose this viral disorder as follows. Bartolo’s sign is related to the ‘Rethiculo–Endothelial–System–Hyperfunction’ (RESH) syndrome (Stagnaro, 1983a, 2004a) which parallels ‘Erythrocyte Sedimentation Rate’ (ESR) and ‘Proteins Electrophoresis’, but it is “more” sensitive and specific than both. In health, a mean intense digital pressure above the sternum midline or iliac crest or skin projection of the spleen brings about a GAR after a latency time (Lt) of 10 seconds as well as a caecal reflex and the spleen decongestion. In practice, physicians evoke just the “vagal” GAR, taking in due account that there are three different types (of varying entity) of RESH, useful both for diagnosis and therapeutical monitoring (Table 2):
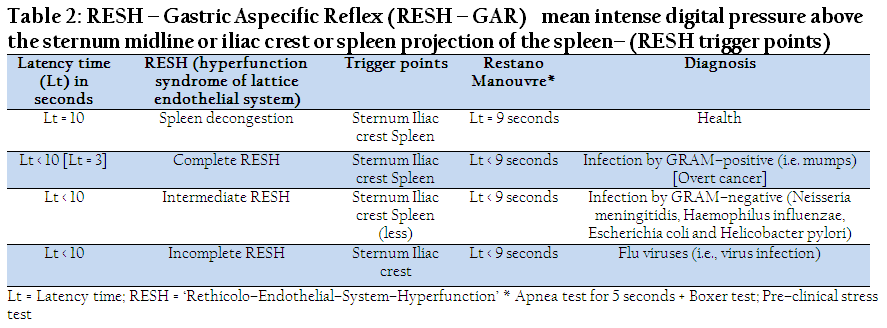
Table 2: RESH – Gastric Aspecific Reflex (RESH – GAR) mean intense digital pressure above the sternum midline or iliac crest or spleen projection of the spleen– (RESH trigger points)
A) Complete RESH: sternum, iliac crest and spleen are GAR trigger points; it occurs characteristically in positive–Gram infections, where Lt decreases to 6 seconds as in nephropathy and in common flu (including parotitis) and malignant cancers (where Lt can decrease even to 3 seconds, and minimal values are observed in overt cancer).
B) Intermediate RESH: spleen is the trigger point of the syndrome, but its stimulation provokes a remarkably lower GAR comparing it with those observed stimulating sternum and iliac crest. This is present in Gram–negative infections as in Neisseria meningitidis, Haemophilus influenzae, Escherichia coli and Helicobacter pylorii infections.
C) Incomplete RESH: spleen is not the trigger point of the syndrome. It needs to stimulate just sternum and iliac crest. This is typical of viral flu.
We underscore here the possibility of easily and quickly recognizing the ‘chronic’ antibodies synthesis in the spleen during flu, as well as the spleen “small” antibody production, in case of Gram–negative bacteria (Escherichia coli, Helycobacter pylorii, Clamidya, etc.), which play a pivotal role in bed–side diagnosis of virus or Gram–negative infections. As a matter of facts, in case of flu– and para–flu–viruses, the spleen antibody synthesis is not increased, as it happens in the sternal marrow, so that Lt of spleen–GAR is physiological, namely 10 seconds. As far as differential diagnosis between Gram + and Gram– infections is considered, only in the first disorders both spleen– and sternal GAR show the same intensity. Typically, in Gram–negative infections (e.g., due to Escherichia coli) Spleen–GAR is significantly lower.
In case of incomplete RESH the spleen is not a trigger–point. Physiologically, it produces antibodies but it does not augment the anti–body synthesis. For the spleen the flu viruses is not an alarm case (it runs physiologically, because there is a hierarchy of psycho–neural–endocrine immune (PNEI) system response). On the other hand, in case of childhood viruses, the spleen reacts intensively as significant trigger–point.
Other QBS reflexes are useful in the daily practice as the bio–entanglement signs (http://www.sisbq.org/le–costituzioni–sbq.html). In short, an intense digital pressure above the sternum midline or iliac crest brings about a simultaneous GAR in case of flu or para–flu viruses. The same manouvre, applied upon the skin projection of spleen does not provoke a simultaneous GAR, for the above–mentioned reasons confirming the diagnosis of incomplete RESH.
In case of bacterial infection, Domenichini’s sign (Stagnaro, 2004a) is useful to distinguish between Gram–negative and Gram–positive. During lung auscultatory percussion and ‘Apnea Test’ in healthy persons the minimal value of vertical diameter of ilo–pulmonary bronco–vasal trunk lasts for exactly 3.5 sec. (reflex duration), in case of viral flu for 7.5 s, in case of Gram–positive for 4.5 s, in case of Gram–negative for 5.5 s. Summarizing, through the QBS clinical method above mentioned, a differential diagnosis of flu viruses and bacteria infection (Table 3) is practically possible, bed–side, just using the stethoscope, through several QBS signs, confirming and consistent each others, as resumed in Table 3.

Clinical evidences show that every diagram phase (Figure 1) is strictly correlated with both function and structure of well–defined parts of different macro– and micro–vascular systems, and their relations, in which some modifications occur during local or systemic morbid processes as studied by Clinical Microangiology (Stagnaro 1985, 1986a, 1986b). Reflex geometric representations (TMU diagrams) are useful “diagnostic” tools in origin, i.e., the trained physician can recognize flu viruses (Figure 1) many hours before the occurrence of well–known clinical signs (really not always present in the classic form), as well as of numerous other QBS signs, when the physician looks for them in a patient at rest (basal values), i.e., without sensitization manoeuvres or dynamic tests. Moreover, when pathological processes are apparently finished, in finger–pulp TMU the typical sign of intense fourth phase persists for about a week, allowing the physician to recognize the former disorder’s nature, even if erroneously considered, both in emergency room and in hospital as well as in the day–to–day practice (large variety of personal cases). As a matter of fact, all physicians have faced a “patient”, apparently not involved by whatever disease, who after some hours began to sneeze, vomit, present with cephalalgia, vertigo and diarrea, finally diagnosed as flu. The knowledge of flu diagram and/or the performance of sensitization manoeuvres of QBS signs allow to avoid such disappointing episodes, although they by themselves are not cause of a patient’s additional injury.
Regarding the differential diagnosis between seasonal flu virus and A/H1N1 a central role is played by the parametric values of BALT– gastric aspecific reflex (GAR), informing about antibody synthesis (Stagnaro, 2009d). In seasonal flu, starting from the contagious, as well as immediately after vaccine injection, Latency time lowers to 4–5 seconds (basal value Lt is 6 seconds) and reflex intensity is 3 cm (basal physiological value is 2 seconds), followed by the characteristic ‘tonic Gastric Contraction’ (tGC). On the contrary, in case of swine flu, latency time is lowest, 2–3 s, while reflex intensity is highest, i.e., 5 cm. In addition, even when gastro–entero–colitis is absent, antibody synthesis in the liver and intestinal lymph–nodules parallels that of BALT.
Summarizing, from these particular “diagnostic” aspects of TMU diagrams, experimental and clinical evidences allow us to state that their routine use during physical examination will provide certainly to doctors a very large amount of information, so that they will be able to direct the successive diagnostic process and to study deeply all diseased biological systems, even in individuals symptomless and apparently healthy. Beside the diagnostic aspect, there is the clinical research, facilitated by the different diagrams, unavoidable in bed–side detecting hemorrheological, vasomotor, biochemical–metabolic and chemical modifications under different situations, physiological as well as during various tests, static and dynamic “clinical” evaluation. Finally, there is the contribution given by the use of various diagrams to therapeutic monitoring, performed at the bed–side in an objective way.
The QBS ‘Flu–dependent Brain X Syndrome’
Metabolic syndrome is a combination of medical disorders that increase the risk of developing cardiovascular disease and diabetes, in about 50% of all cases. It is also known as metabolic X syndrome, X syndrome, insulin resistance syndrome, Reaven's syndrome. The pre–metabolic syndrome, as defined by one of the authors, is the syndrome that precedes the metabolic one, and is linked with congenital real risks and their related QBS constitutions (Stagnaro et al. 2004b, 2005, 2009a; Stagnaro, 2007a). With the aid of QBS method one of the authors discovered one more syndrome, termed ‘Flu–dependent Brain X Syndrome’, connected with the well–known heart X Syndrome.
Through ‘Brain Sensor Bedside Evaluation’ (BSBE) (Stagnaro et al. 2011, 2012) we can see that the ‘Brain Sensor’ is always activated both in case of Labirintosis and ‘Flu–dependent Brain X Syndrome’. How to distinguish the one from the other? In case of Labirintosis there is type I, associated Microcirculatory Activation (MA) located in Auricolo–Vestibolar sites, whose skin projection area is in the temporal area (both right and left side), practically 5 cm over the external auditory meatus, i.e., over the GH neural centre.
In turn, in ‘Flu–dependent Brain X Syndrome’ there is a significant cerebral oedema (presence of cistic – GAR, brought about by digital pressure on the cranium, ureteral reflex in toto and choledocic reflex) if the four involved areas are stimulated (the first sign, is expression of an augmented volume of the interstitium from incremented capillary permeability and from an altered ratio of free–bound water). Finally, due to the infective–inflammatory nature of ‘Flu–dependent Brain X Syndrome’, both PCR reflex and cytokine reflex are present. In fact, the nail (finger pulp) pressure provokes the GAR after a Lt less than the physiological 10 seconds, inversely related to the severity of ‘Flu–dependent Brain X Syndrome’.
‘Flu–dependent Brain X Syndrome’ has an inflammatory nature evidenced by the ‘QBS Microcirculatory Disturbances of Brain’, that physician can observe in frontal–parietal– and occipital cerebral regions, but not in cerebellum convolutions, type I, associated microcirculatory activations, which last intense for some minutes, and then slowly disappear in about 24 hours. Importantly from the ethiological view–point, during ‘Flu–dependent Brain X Syndrome’, ungual pressure applied upon frontal–, parietal–, and occipital–regions brings about gastric aspecific reflex after a latency time lower than the physiological 10 s, indicating the inflammatory nature of the syndrome.
DIAGNOSIS OF ‘FLU–DEPENDENT BRAIN X SYNDROME’
We have performed a clinical experimental research enrolling 10 white individuals in the age between 21 and 45 years, Females 6 and Male 4, clinically observing them, with the aid of QBS method, during flu epidemics, discovering a new syndrome, termed ‘Flu dependent Brain X Syndrome’ caused by flu viruses. Among the several QBS signs of flu diagnosis, we considered the finger pulp microcirculatory diagram of flu, as above illustrated (Figure 1).
To understand the patho–physiology of the ‘Flu dependent Brain X Syndrome’, physicians must take into account what has already been discovered and described by one of the authors (Stagnaro 1983b, 1986c, 2007), i.e., the ‘Acute Benign Variant Polymyalgia Rheumatica’ (ABVPR), characterized by a polymyalgia like symptomatology, associated with localised, dull, thoracic ache, brought about by flu viruses in individuals, mainly female, positive for rheumatic QBS constitutions (Stagnaro, 1983b).
In the recruited subjects, flu viruses caused intense BALT impairment, with the exception of a single BALT, whose activity (size) was significantly increased, like the antibody synthesis, as the local type I, associated, microcirculatory activation demonstrates (Stagnaro 1983b, 1986c, 2004a). As a working hypothesis, analogously to ABVPR, we suppose that the brain antibody synthesis, termed ‘Cerebral Associated Lymphatic Tissue’ (CALT), discovered by one of the authors (Stagnaro, 2004a), can be altered in the initial stage of flu episode. As in ABVPR, even in the involved brain areas sites of CALT, there is a small brain oedema, revealed by a cystic syndrome QBS diagnosed by ‘in toto’ ureteral–, choledocic–, and gastric aspecific reflexes, which appear during mean intense digital pressure, applied upon skin projection areas of frontal–parietal–occipital cerebral convolutions.
The initial sign of ‘Flu dependent Brain X Syndrome’ is the cerebral acidosis always induced by the flu viruses, with an augmented ratio of free to bound water/ which increases the interstitium. This fact provokes a slight cerebral oedema, revealed by a vasomotion activation (vasomotility + vasomotion). Its slow fluctuations (interstitium alterations are an obstacle for microvessels walls dynamics) cause a very slow re–modeling returning to the physiological cerebral histangium.
In the clinical symptomathology of ‘Flu dependent Brain X Syndrome’ there is a type I, associated, microcirculatory activation (vasomotility and vasomotion rise to about 8 seconds, while the normal value (NN) is 6 seconds), but likely as reaction to the existing light cerebral oedema caused by the flu viruses as it happens in Finger Pulp TMU (Figure 1). In fact, the interstitial free water augments and creates an obstacle slowing the microvessels’ fluctuations, therefore pH diminishes: the latency time (Lt) is just 7 seconds instead of the basal 8 seconds, while the reflex duration rises to 5–6 seconds.
Interestingly, in ‘Flu dependent Brain X Syndrome’ the glycocalyx activity is compromised and the latency time (Lt) of ‘Evoked Cerebral Potentials’ significantly rises, corroborating the internal and external consistency of QBS theory (Stagnaro 1983b, 1986c, 2007).
CONCLUSIONS
By means of QBS method, there is the possibility of clinically recognizing the “chronic” antibodies synthesis in the spleen during flu, as well as the spleen “small” antibody production, characteristic of Gram–negative bacteria. This plays a pivotal role in bed–side differential diagnosis between virus and Gram–negative infections. Moreover, interestingly, physicians can now–a–day observe clinically, and in a “quantitative” way, the so–called RESH.
Interestingly, this paper shows how to recognize at the bed–side, really early, an infection, viral in origin, and how to differentiate it from bacterial infection.
As a matter of fact, most adults, and children, of course, with acute bronchitis, consulting their General Practitioner, they will be given antibiotics, although in many cases antibiotics do not modify the natural course of the disorder, at all. The real problem is to recognize “clinically” both the nature of the infectious disorder and the patient's actual defence, including antibody and PCR synthesis: first, the “ethiological”, complete bedside diagnosis and, then, the proper therapy. Finally, the discovery of QBS ‘Flu dependent Brain X Syndrome’ opens new perspectives in differential diagnosis between flu and para–flu viruses. Further researches on larger scale are necessary.
ACKNOWLEDGEMENTS
Our special acknowledgements to Prof. Luca Obertello and Dr. Marco Marchionni who helped us revising the English version of this manuscript.
REFERENCES
Bellmann-Weiler R, Beikircher B, Kurz K, Theurl I and Weiss G (2011). Accuracy of bedside antigen tests in the diagnosis of new influenza A/H1N1v infection. Clin Microbiol Infect. 2011 Feb;17(2):235-7.
http://dx.doi.org/10.1111/j.1469-0691.2010.03235.x
PMid:20384708
Chertow DS and Memoli MJ (2013). Bacterial coinfection in influenza: a grand rounds review. JAMA. 2013 Jan 16; 309(3): 275-82. Hatchette TF, Bastien N, Berry J, Booth TF, Chernesky M, Couillard M, et al (2009). The limitations of point of care testing for pandemic influenza: what clinicians and public health professionals need to know. Can J Public Health. 2009 May-Jun;100(3):204-7.
Hauge SH, Dudman SG, Borgen K, Hungnes O, Brantsaeter A, Iversen B and Aavitsland P (2009). Disease caused by the new influenza A(H1N1) virus. Tidsskr Nor Laegeforen. 2009 Sep 10;129(17):1736-9.
http://dx.doi.org/10.4045/tidsskr.09.0748
PMid:19756053
Jacobus CH and Raja AS (2012). How accurate are rapid influenza diagnostic tests? Ann Emerg Med. 2013 Jan;61(1):89-90.
Jernigan DB, Lindstrom SL, Johnson JR, Miller JD, Hoelscher M, Humes R et al (2009). Detecting 2009 pandemic influenza A (H1N1) virus infection: availability of diagnostic testing led to rapid pandemic response. Clin Infect Dis. 2011 Jan 1;52 Suppl 1:S36-43.
Kawachi S, Matsushita T, Sato T, Nunoi H, Noguchi H, Ota S, et al (2009). Multicenter prospective evaluation of a novel rapid immunochromatographic diagnostic kit specifically detecting influenza A H1N1 2009 virus. J Clin Virol. 2011 May;51(1):68-72.
Moreno R and Rhodes A (2011). From the bedside to the bench: how to improve the care of critically ill pregnant patients with influenza. Crit Care Med. 2011 May;39(5):1199-200.
http://dx.doi.org/10.1097/CCM.0b013e31820e80f5
PMid:21610574
Stagnaro S (1983a). Sindrome percusso-ascoltatoria di Iperfunzione del Sistema Reticolo-Istiocitario Min. Med. 74, 479 [Medline].
Stagnaro S (1983b). Auscultatory Percussion of Rheumatic Diseases. X European Congress of Rheumatology, 26 June-July Moscow, Russian Federation: 175.
PMid:6835586
Stagnaro S (1986a). Auscultatory Percussion Therapeutic Monitoring and Cerebral Dominance in Rheumatology. 2nd World Congress of Inflammation, Antirheumatics, analgesics, immunomodulators. Abstracts, A. Book 1, pg. 116, March 19-22, 1986, Montecarlo.
Stagnaro S (1986b). Valutazione percusso-ascoltatoria della microcircolazione cerebrale globale e regionale. Atti, XII Congr. Naz. Soc. It. di Microangiologia e Microcircolazione. 13-15 Ottobre, Salerno,Italy and Acta Medit. 145, 163.
Stagnaro S and Stagnaro-Neri M (2004a). Introduzione alla Semeiotica Biofisica. Il Terreno oncologico". Ed. Travel Factory SRL., Roma, Italy: 21-32; 203-218.
Stagnaro S and Stagnaro-Neri M (2004b). Le Costituzioni Semeiotico- Biofisiche. Strumento clinico fondamentale per la prevenzione primaria e la definizione della Single Patient Based Medicine. Travel Factory, Roma, Italy: 21-30.
Stagnaro S and Stagnaro-Neri M (2005). Single Patient Based Medicine. La Medicina Basata sul Singolo Paziente: Nuove Indicazioni della Melatonina. Ed. Travel Factory, Roma, Italy: 13-37.
Stagnaro S (2007a). Epidemiological evidence for the non-random clustering of the components of the metabolic syndrome: multicentre study of the Mediterranean Group for the Study of Diabetes. Eur J Clin Nutr.[Medline].
http://dx.doi.org/10.1038/sj.ejcn.1602668
PMid:17299468
Stagnaro S (2007). Polymyalgia Rheumatica and Giant Cell Arteritis: First of All, Early Diagnosis! Ann. Intern. Med. 2007; 146: 631-639 http://www.annals.org/cgi/eletters/146/9/631
Stagnaro S and Singh RB (2009a). Influence of Nutrition on the pre-metabolic syndrome and vascular variability syndrome. Editorial, the Open Nutrition Journal. Bentham Sci. Publish. PMid:19484586
Stagnaro S (2009b). Quantum-Biophysical-Semeiotic Bedside Diagnosis of Flu, since its earliest stage. 30 October, 2009. CMAJ 2009; 181: E195- 196E. http://www.cmaj.ca/content/181/9/E195.figures-only/reply#cmaj_el_228652
Stagnaro S (2009c). Flu Bedside Diagnosis and Differential Diagnosis. BNJ. Rapid Response. http://www.bmj.com/rapid-response/2011/11/02/flu-bedside-diagnosis-and-differential-diagnosis
Stagnaro S (2009d). Subjects at Inherited Real Risk of A/H1N1 broncho- pneumonitis. Medical Page. Comments. 4/11/09 http://www.medpagetoday.com/comments.cfm?tbid=16786
Stagnaro S and Caramel S (2011). Right Planum Temporale Dominance, Congenital Acidosic Enzyme- Metabolic Histangiopathy, Quantum Biophysical Semeiotic Constitutions-Dependent Inherited. 11 May, 2011. Shipu.com http://wwwshiphusemeioticscom-stagnaro.blogspot.com/2011/05/right-planum-temporale-dominance.html
Stagnaro S and Caramel S (2012). New ways in physical Diagnostics: Brain Sensor Bedside Evaluation. The Gandolfo's Sign. – JOQBS. Available at: http://www.sisbq.org/uploads/5/6/8/7/5687930/bsbe.pdf
Talbot HK, Williams JV, Zhu Y, Poehling KA, Griffin MR and Edwards KM (2010). Failure of routine diagnostic methods to detect influenza in hospitalized older adults. Infect Control Hosp Epidemiol. 2010 Jul;31(7):683-8.
http://dx.doi.org/10.1086/653202
PMid:20470035 PMCid:PMC3715378
Yasuda C, Sovann L, Kasper M, Williams M and Wierzba TF (2012). Epidemiological characteristics, clinical presentation and diagnosis at point-of-care during the first wave of the H1N1 influenza pandemic in Cambodia. Southeast Asian J Trop Med Public Health. 2012 Jan;43(1):68-77
PMid:23082556



