Journal of Infection and Molecular Biology
Research Article
Journal of Infection and Molecular Biology 1 (1): 13 – 17Antimicrobial Sensitivity Pattern of Methicillin Resistant Staphylococcus aureus Isolated from Hospitals of Kohat District, Pakistan
Mubbashir Hussain1*, Abdul Basit1, Abdullah Khan1, Kashif Rahim1, Asad Javed1, Asif Junaid1, Shahzad Munir1, Hamid Rasul Niazi1, Muhammad Sohail1, Tassadaq Hussain2,
- Department of Microbiology, Kohat University of Science and Technology
- Qarshi Research International Labs, Haripur, Pakistan
*Corresponding author:mubashirbangash@gmail.com
ARTICLE CITATION:
Hussain M, Basit A, Khan A, Rahim K, Javed A, Junaid A, Munir S, Niazi HR, Sohail M, Hussain T (2013). Antimicrobial sensitivity pattern of methicillin resistant Staphylococcus aureus isolated from hospitals of Kohat district, Pakistan. J. Inf. Mol. Biol. 1: 13 – 17.
Received: 2013-02-21, Revised: 2013-03-03, Accepted: 2013-03-09
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/2/19/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The study was conducted to determine prevalence and analyze antibiotic susceptibility patterns of Methicillin Resistant Staphylococcus aureus (MRSA) isolates in two hospitals of District Kohat, Khyber Pakhtunkhwa province, Pakistan. Staphylococcus strains (n = 434) comprising of 191 (44 %) MRSA and 243 (56 %) coagulase negative were isolated from different clinical samples and identified using conventional microbiological procedures. Majority of the isolates (15.55%) were identified from surgical ward followed by outdoor patient department (OPD, 14.70%). The percentage of MRSA in wound samples was highest (24.08 %) followed by pus samples (21.46 %) and vaginal swab (3.14 %). MRSA strains (n = 191) isolated from two hospitals of Kohat were resistant to amoxycillin (100%), followed by cefotaxime (76.43 %), ofloxacin (74 %), levofloxacin (70.15 %), erythromycin (69.10 %) and chloramphenicol (34.03 %). Highest sensitivity was found against vancomycin (99.55 %). A potentially alarming prevalence and multi drug resistance pattern found in MRSA isolates indicates major health concerns in remote district Kohat.
INTRODUCTION
Hospital associated methicillin resistant Staphylococcus aureus (HA-MRSA) is emergence of MRSA from the patients having current or recent hospitalization, receives dialysis, or resides in a long-term care facility (Milyani and Ashy, 2012). MRSA has become a leading cause of nosocomial infections worldwide since the first European isolate of MRSA detected in 1960s (Lowy, 1998; Tristan et al., 2007). During the period 1970 to 2010, outbreaks of hospital acquired infections of MRSA were observed around the world including Saudi Arabia (Madani et al., 2001), Austria (Krziwanek et al., 2009), Argentina (Reyes et al., 2009), South Africa (Shittu et al., 2009), Italy (Soavi et al., 2010). These outbreaks were mostly associated with neonatal, intensive care and burns units (Liu et al., 2011).
MRSA shows resistance to multiple antibiotics such as gentamicin, norfloxacin, fucidic acid, erythromycin and clindamycin (Shai et al., 2004). Infections caused by resistant MRSA are prominent threat to animal and human health. Infection outbreaks have been reported from burn wards, nurseries, intensive care units as well as in clinical and surgical patients and due to misuse of antibiotics, lack of hand washing, irresponsible nursing care and presence of carriers among the hospital staff (Zermina et al., 2012). There are two types of Staphylococcus aureus found in nosocomial environments: permanent and transitory. The former can be found on healthcare workers and in the hospital environment (Yao et al., 2010; Persoons et al., 2009, Shai et al., 2004). These infection has also been reported in different animal species such as sheep, goat, cows, dogs (Bassim and El-Maghraby, 2005) and hospitalized horses (Hartmann et al., 1997)
In developing countries like Pakistan, antibiotic resistant bacteria are persistent challenge and difficult to control because of irrational use of antibiotics. There exists a paucity of data regarding MRSA in Khyber Pakhtunkhwa, province of Pakistan. The present study, therefore, has been conducted for the first time to investigate the antibiotic susceptibility profiles of MRSA isolated from human population in district Kohat, Pakistan.
MATERIALS AND METHODS
Sampling
From January to December 2012, a total of 552 samples were collected from different wards (OPD, Ear Nose and Throat (ENT), Medical, Burns, Orthopedic, Surgical, Children, Gynaecological ward and Main Operation Theater) of Liaqat Memorial hospital and DHQ hospital KDA district Kohat (Khyber Pakhtunkhwa) Pakistan. These samples were collected from patients admitted in different wards of above said hospitals with history of different clinical problems. Samples included whole blood, pus, wound swabs, throat swabs, sputum, high vaginal swab (HVS) and urine samples. Samples were labeled accordingly and were subjected to screening of Staphylococcus aureus and subsequent antimicrobial susceptibility.
Isolation of S. aureus from clinical samples
Staphylococcus aureus was isolated from each sample as per protocol produced. Each sample was inoculated onto Mannitol Salt Agar (MSA) (Oxoid, UK) followed by identification of S. aureus on the basis of Gram staining reaction and biochemical tests such as catalase, coagulase and DNase tests as discussed previously by Perveen et al., (2013).The positive results of these tests were considered to be the positive isolates of S. aureus.
MRSA screening
Methicillin was used to screen S. aureus isolates for presence of methicillin resistance. Briefly, each isolate was streaked on surface of Muller-Hinton agar (Oxoid UK) containing 6 µg/ml of methacillin and incubated at 37 °C for 24 hours as performed previously (Ma et al., 2007). Isolates showing growth on this media were preserved and labeled as MRSA for further studies.
Anti-biogram Assay
The Kirby-Bauer disc diffusion method was used to evaluate the antimicrobial susceptibility pattern of the MRSA isolates against different commonly used antibiotics.
Amoxicillin (60 µg), cefotaxime (20 µg), cephradin (30 µg), chloramphenicol (30 µg), ciprofloxacin (5 µg), doxycycline (1µg), gentamicin (10 µg), levofloxacin (5µg), ofloxacin (10 µg), sparfloxacin (20 µg), norfloxacin (5 µg) and vancomycin (30 µg) (Oxoid UK), were used in the present study.
and the results were interpreted by measuring zone of inhibitions according to standard guidelines as described by Perveen et al. (2013).
RESULTS
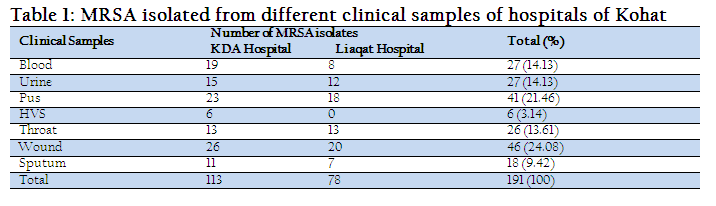
Out of 552 samples tested, we isolated 434 Staphylococcus strains containing 191 (44 %) MRSA and 243 coagulase negative Staphylococcus strains, while rest of the samples (109) were negative for Staphylococcus. Out Of these Staphylococcus positive samples, 51.79% were from male patients while remaining 48.21% were from female patients. Statistically there was no difference (P > 0.05) in prevalence of MRSA on sex and age basis (data not shown). Isolates were mostly taken from surgical ward (15.55%) followed by OPD (14.70 %). Highest percentage of MRSA was isolated from wound swabs (24.08 %) followed by pus samples (21.46 %) while the lowest percentage of MRSA was from HSV (3.14 %). Isolation of MRSA from clinical samples is detailed in Table 1.
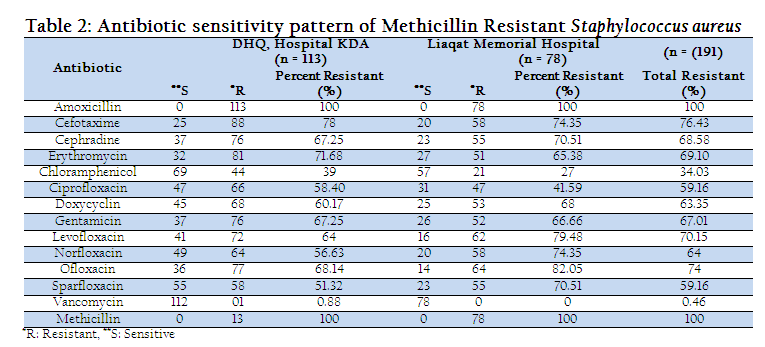
The antibiotic sensitivity patterns of MRSA isolated from clinical specimens were found to be highly variable. All the 191 MRSA strains isolated from two hospitals of Kohat were resistant to methicillin (used for screening) and penicillin (100%), followed by cefotaxime (76.43 %),ofloxacin (74 %), levofloxacin (70.15 %), erythromycin (69.10 %) and chloramphenicol (34.03 %). Highest sensitivity was found against vancomycin (99.55 %). The antimicrobial susceptibility pattern of MRSA isolates against different classes of antibiotics is shown in Table 2.
DISCUSSION
The results of present study showed that the prevalence MRSA in clinical samples from two government hospitals was 44 %. Previous reports have showed variable prevalence of MRSA strains among various cities of Pakistan including 61% in Lahore, 57% in Karachi, 46% in Rawalpindi and 54 % in Peshawar (Ahmad et al. 2000, Hafiz et al. 2002, Qureshi et al. 2004, Shafiq et al. 2011). This raised isolation of MRSA with the passage of time may be attributed to the transfer of resistance genes between bacterial cell and persistence of bacteria in hospital environment due to antibiotic resistance (Saima et al. 2007). Absence of control program for antibiotics usage pattern is another factor which facilitates MRSA to increase in concentration (Hacek et al., 1999). In present study statistically no significant difference was observed in prevalence of MRSA on sex and gender basis that is in accordance with previous studies conducted by Khatoon et al., (2002).
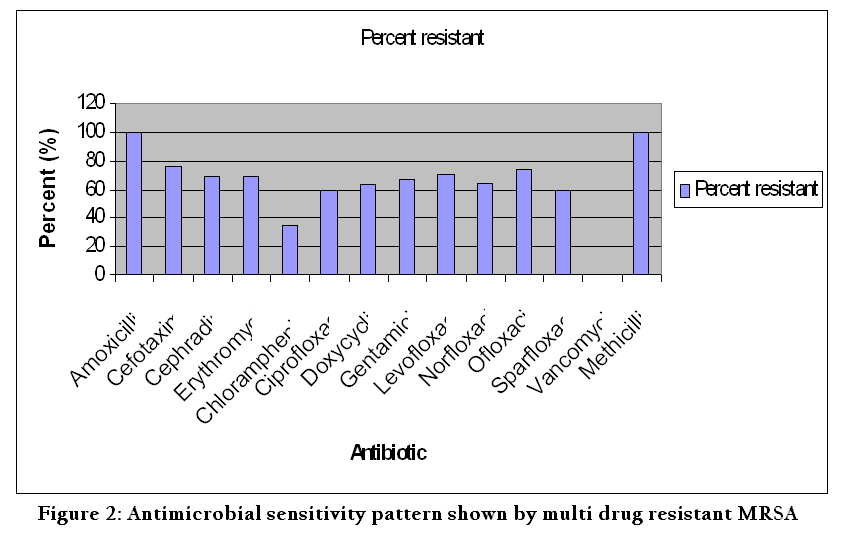
The results of present study showed multiple drug resistance of MRSA strains isolated from two hospitals of Kohat as shown in figure 2. We have shown that all 191 MRSA strains were 100% resistant to methicillin and amoxycillin. The resistance pattern of methicillin and amoxycilline observed against MRSA was similar to what has been reported from other part of the world. Zermina et al., 2012 conducted study in Rawalpindi and found 92% of MRSA were resistant to Ampicillin. Amoxycillin, a derivative of penicillin, has been in use for last two decades, so development of high resistance is obvious. In present study 68.58 % and 76 % of MRSA strains showed resistance against cephradine and cefotaxime respectively. James and Reeves (1996) described that MRSA strains are resistant to first, second, third and fourth generation of cephalosporins. In a study conducted by Perveen et al. (2013), 83% of the MRSA showed resistance against cephradine whereas Mahmood et al. (2001) reported 29% resistance of generation cephalosporins. In this study, we have examined that67.01% MRSA showed resistance against gentamicin that is lower than the 76.35% of MRSA resistance towards gentamicin as described by Perveen et al. (2013). Gentamicin is an aminoglycoside and is most often prescribed because of its low cost and synergistic activity with ß-lactum antibiotics (Hafiz et al., 2002). In this study 69.10 % of MRSA were resistant to erythromycin, which isin accordance with previous reports conducted by Perveen et al. (2013). Among quinolones the percentage resistance found in MRSA in present study was quite higher (ciprofloxacin (59.16), ofloxacin (74 %), levofloxacin (70.15 %). Previously reported resistance of ciprofloxacin and other quinolones also showed higher pattern as reported by Auckenthaler et al. (2000), Zermina et al. 2012. The development of S. aureus resistance to ciprofloxacin might be due to previous antimicrobial chemotherapy of patient before hospitalization. When quinolones are used to treat infections caused by other bacterial pathogens, S. aureus colonized on these patients (e.g., on their skin or mucosal surfaces) are likely to be exposed to sub therapeutic antibiotic doses and are therefore at risk of developing resistance. These resident, resistant strains then become the reservoir for future infections (Mandell, 2005). We observed that all MRSA isolates gave 99.55 % sensitivity to vancomycin. There was only one isolate that was found to be resistant to vancomycin. These results coincide with the findings of multi drug resistance in the study conducted by Perveen et al. (2013). It is well known that emergence of bacterial resistance is promoted by excessive use of antibiotics. The presence of antibiotics residues in livestock products like milk and meat could be another responsible for maintaining resistant strains in environment (Persoon et al., 2009). The healthcare workers inserted in this epidemic chain have great importance in the increasing resistance of contaminants, serving as a source of transmission and information for empirical prescription of antibiotics.
The results of present study clearly showed high prevalence of MRSA in hospitals of district Kohat. The antibiotics used in this study are frequently prescribed by clinicians without carrying out anti-biogram assays on samples of their patients. Moreover, common people have easy access to these antibiotics available to them at local pharmacies without any prescriptions from doctors. Therefore, the rise in resistance is clearly due to irrational use of antibiotics and non existence of protocols and guidelines for safe practice in terms of treatment of MRSA.
CONCLUSION
MRSA were isolated in high concentration from clinical samples in Kohat and showed a high risk to the patients and staff working in the hospital. The overcrowding in hospital, lack of facilities and lack of knowledge about HA-MRSA result in the presence of nosocomial pathogen in high concentration. MRSA strains isolated showed resistance to multiple antibiotics. We suggest an implementation of preventive measure in order to minimize the bacterial resistance to antibiotics. An electronic record of antibiotic usage should be made to prevent unnecessary usage of broad spectrum antibiotics and increase recommended usage of antibiotics. All health care personnel should strictly follow the preventive guideline for patient as well as for their own safety. Proper antibiotics susceptibility test should be made for all suspected infection caused by MRSA. Vancomycin showed good results against MRSA in the present study. But the prescription of this antibiotic should be limited and subjected to presentation of proper antimicrobial sensitivity assay reports.
ETHICAL CONSIDERATION
The samples were obtained from patients with prior informed consent and explaining to them the importance of this study. The study was finally approved by Research and ethical committee, Department of Microbiology, Kohat University of Science and Technology, Pakistan.
CONFLICT OF INTEREST
The authors declare no conflict of interest of any type.
ACKNOWLEDGEMENTS
We are grateful to Dr. Younas Nadeem and Dr Sami, DHQ hospital Kohat for their technical help in obtaining clinical samples from patients. We also express our thanks to laboratory staff in the Department of Microbiology, Kohat University for facilitating us in providing sterilized glassware and other requirements during the study period. Lastly, we are thankful to all patients for providing the clinical samples for present study.
REFERENCES
Ahmed A, Qureshi SF and Ansari N (2000). Prevalence and antibiotic sensitivity pattern of methicillin resistant Staphylococcus aureus (MRSA) infection in a tertiary care hospital. Karachi: Liaquat National Hospital Symposium.
Auckenthaler R, Courvalin P, Feger C and Roche G (2000). In vitro activity of quinupristin/ dalfopristin in comparison with five antibiotics against worldwide clinical isolates of staphylococci.Clin. Microbiol. Infect. 6: 608 - 612.
http://dx.doi.org/10.1046/j.1469-0691.2000.00152.x
PMid:11168064
Bassim H and El-Maghraby M (2005). Methicillin-resistant Staphylococcus aureus (MRSA) a challenge for infection control. ASJOG. 2: 277 - 279.
Boyce JM (1990). Increasing prevalence of methicillin-resistant Staphylococcus aureus in the United States. Infect. Contr. Hosp. Epidemiol. 11: 639 - 642.
http://dx.doi.org/10.1086/646114
http://dx.doi.org/10.2307/30146866
PMid:2273227
Hacek DM, Suriano T, Noskin G, Kruszynski J, Reisberg B and Peterson L (1999).Medical and economic benefit of a comprehensive infection control program that includes routine determination of microbial clonality.Am. J. Clin. Pathol. 111: 647 - 654.
PMid:10230355
Hafiz S, Hafiz AN, Ali L, Chughtai AS, Memon B, Ahmed A, et al. (2002). Methicillin resistant Staphylococcus aureus: a multicentre study. JPMA. 52: 31 - 32.
Hartmann FA, Trostle SS and Klohnen AAO (1997). Isolation of methicillin-resistant Staphylococcus aureus from a postoperative wound infection in a horse. J. Am. Vet. Med. Assoc. 211: 590 - 592.
PMid:9290826
Helena BS, Machado DP, Camey SA, Uchenbecker RS, Barth AL and Wagner MB (2010). Prevalence and acquisition of MRSA amongst patients admitted to a tertiary-care hospital in Brazil. BMC Infect. Dis. 328(10): 1 - 7.
James PA and Reeves DS (1996). Bacterial resistance to cephalosporins as a function of outer memberane permeability and access to their target.J Chemother. 8: 37 - 47.
PMid:8738845
Khatoon N, Bukhari H, Riaz JR and Sheikh AS (2002).Prevalence of methicillin resistant staphylococcus aureus (MRSA) infection laboratory study at Mayo Hospital Lahore.Biomedica. 18: 49 - 52.
Krziwanek K, Metz-Gercek S and Mittermayer H (2009). Methicillin-resistant Staphylococcus aureus ST398 from human patients, upper Austria.Emerg. Infect. Dis. 15(5): 766 - 769.
http://dx.doi.org/10.3201/eid1505.080326
PMid:19402964 PMCid:PMC2687006
Liu C, Bayer A, Cosgrove S, Daum RS, Fridkin S, Gorwitz R, Kaplan S, Karchmer A, Levine D, Murray B, Rybak M, Talan D and Chambers H (2011). Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus.Infections in Adults and Children. Downloaded from cid.oxfordjournals.org by guest on November 4.
Lowy FD (1998).Staphylococcus aureus infections.New. Eng. J. Med. 339: 520 - 532.
http://dx.doi.org/10.1056/NEJM199808203390806
PMid:9709046
Ma SH, Lee YS, Lee SH, Kim HK, Jin JS, Shin EK and Lee JC (2007). Methicillin-resistant Staphylococcus aureus clones with distinct clinical and microbiological features in Korean community. J. Med. Microbiol. 56(6): 866 - 868.
http://dx.doi.org/10.1099/jmm.0.46962-0
PMid:17510277
Madani TA, Al-Abdullah NA, Al-Sanousi AA, Ghabrah TM, Afandi SZ and Bajunid HA (2001). Methicillin-resistant Staphylococcus aureus in two tertiary care centers in Jeddah, Saudi Arabia. Infect. Cont. Hosp. Epidemiol. 22: 211 - 216.
http://dx.doi.org/10.1086/501891
PMid:11379711
Mahmood A, Rafique S, Qayyum M and Qazilbash AA (2001). Prevalence of nosocomial and community-based methicillin-resistant Staphylococcus aureus (MRSA).Pak. J. Med. Res. 40: 86 - 89.
Mandell GL, Bennett JE and Dolin R (2005). Eds. Principles and practice of infectious diseases.6th ed. Churchill Livingstone, London.
Milyani R and Ashy N (2012). Inhibitory effect of some plant extracts on clinical isolates of Staphylococcus aureus. Afr. J. Microbiol. Res. 6(40): 6822 - 6829.
Persoons D, Hoorebeke SV, Hermans K, Butaye P, Kruif AD, Haesebrouck F and Dewulf J (2009). Methicillin-resistant Staphylococcus aureus in poultry.Emerg. Infect. Dis. 15(3): 452 - 453.
http://dx.doi.org/10.3201/eid1503.080696
PMid:19239762 PMCid:PMC2666289
Perveen I, Majid, A, Kanwal S, Naz I, Sehr S, Safia A and Muhammad AR (2013). Prevalence and antimicrobial Pattern of Methacillin resistant Staphylococcus aureus and Coagulase negative Staphylococcus in Rawalpindi, Pakistan. British J. of Med & Med. Res. 3(1): 198 - 209.
http://dx.doi.org/10.9734/BJMMR/2013/2109
Qureshi A, Rafi HS, Qureshi SM and Ali AM (2004) The current susceptibility patterns of methicillin resistant Staphylococcus aureus to conventional anti staphylococcus antimicrobials at Rawalpindi. Pak. J Med Sci. 20(4): 361 - 364.
Reyes J, Rincon S, Diaz L, Panesso D, Contreras GA, Zurita J, Carrillo C, Rizzi A, Guzman M, Adachi J, Chowdhury S, Murray BE and Arias CA (2009). Dissemination of methicillin-resistant Staphylococcus aureus USA300 sequence type 8 lineage in Latin America.Clin. Infect. Dis. 49: 1861 - 1877.
http://dx.doi.org/10.1086/648426
PMid:19911971 PMCid:PMC2787674
Samia P, Barakzi Q, Farooqi BJ, Nazia K and Sabir N (2007). Antimicrobial susceptibility pattern of clinical isolates of methicillin resistant Staphylococcus aureus. J. Pak. Med. Asso. 57(1): 2 - 4.
Shafiq R, Shahina M, Ahmad JM, Syed HS and Malala R (2011).Incidence of Methicillin reistant Staphylococcus in Peshawar.J. Ayub. Med.CollegeAbbotabad, 23:1.
Shagufta N and Jayaraj YM (2010). Nasal carriage of methicillin-resistant staphylococcus aureus isolated from intensive care unit patient. Res. J. Boil. Sci. 5(2): 150 - 154.
http://dx.doi.org/10.3923/rjbsci.2010.150.154
Shai A, Natalya MD, Bilenko MD, Zeev RB and Halevy MD (2004). Use of infection control procedures in an out-patient clinic for leg ulcers and the rate of contamination with methicillin-resistant Staphylococcus aureus. Wounds. 16(6): 15 - 25.
Shittu A, Nubel U, Udo E, Lin J and Gaogakwe S (2009). Characterization of meticillin-resistant Staphylococcus aureus isolates from hospitals in Kwazulu-Natal province, Republic of South Africa. J. Med. Microbiol. 58: 1219 - 1226.
http://dx.doi.org/10.1099/jmm.0.011452-0
PMid:19528149
Siddique GM, Karamat KA and Hannan A (1999). Prevalence of methicillin resistant staphylococcus aureus: a study at PAF Hospital Sargodha. Pak. J. Pathol. 10: 26 - 28.
Soavi L, Stellini R, Signorini L, Antonini B, Pedroni P, Zanetti L, Annalisa M, Alberto P, Angelo P and Carosi G (2010). Methicillin-resistant Staphylococcus aureus ST398, Italy.Letters, Emerg. Infect. Dis. 16(2): 346 - 348.
http://dx.doi.org/10.3201/eid1602.091478
PMid:20113580 PMCid:PMC2958030
Tristan A, Bes M, Meugnier H, Lina G, Bozdogan B, Courvalin P, Reverdy ME, Enright MC, Vandenesch F and Etienne J (2007). Global distribution of Panton-Valentine leukocidin-positive methicillin-resistant Staphylococcus aureus.Emerg. Infect. Dis. 13(4): 594 - 600.
http://dx.doi.org/10.3201/eid1304.061316
PMid:17553275 PMCid:PMC2725977
Yao D, Yu FY, Qin ZQ, Chen C, He SS, Chen ZQ, Zhang XQ and Wang L (2010). Molecular characterization of Staphylococcus aureus isolates causing skin and soft tissue infections (SSTIs). BMC Infect. Dis. 10: 133 - 137.
http://dx.doi.org/10.1186/1471-2334-10-133
PMid:20500885 PMCid:PMC2889999
Zermina R, Kalsoom F, Abdul S and Murtaza G (2012) Prevalence of nasal Staphylococcus aurues and Methicillin resistant Staphylococcus aureus in hospital personnela and associated risk factors. ActaPoloniaePharmaceutica - Drug Research, 69: 985 - 991.



