Journal of Infection and Molecular Biology
Short Communication
Journal of Infection and Molecular Biology. 1 (4): 67 – 70Multiple Drug Resistance Pattern in Urinary Tract Infection Patients in Peshawar, Khyber Pukhtunkhwa (KPK) Province, Pakistan
Khawar Ali Shahzad1*, Fahim Ullah1, Khushi Muhammad2, Farzana Khatoon1, Mahmood Ul Hassan Qazi1, Ishfaq Ahmed1
- Institute of Molecular Biology and Biotechnology, The University of Lahore, Lahore, Pakistan
- Department of Microbiology, Faculty of Veterinary Science, University of Veterinary and Animal Sciences, Lahore, Pakistan
*Corresponding author:khawar7bar@yahoo.com
ARTICLE CITATION:
Shahzad KA, Ullah F, Muhammad K, Khatoon F, Qazi MH and Ahmed I (2013). Multiple drug resistance patterns in urinary tract infection patients in Peshawar, Khyber Pukhtunkhwa (KPK), Pakistan. J. Inf. Mol. Biol. 1 (4): 67 – 70.
Received: 2013–07–16, Revised: 2013–11–20, Accepted: 2013–11–27
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/2/148/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Urinary tract infection (UTI) is the most common problem in hospitalized and outdoor patients. It is mainly found in females because of the shortness of the urethra and closeness to anus, which facilitate entrance of fecal micro–flora to urinary tract. Aim of the study was to investigate the bacterial uro-pathogens and their antibiotic susceptibility in a tertiary care hospital, Peshawar, Pakistan. Urine samples (n = 200) were analyzed and cultured on cysteine lactose electrolyte deficient (CLED) medium. All the bacterial isolates were identified by conventional biochemical tests. Of the total, bacteria were isolated from 113 patients. In positive samples, 36 (31.9%) were male and 77 (68.1%) were female, whereas, 80 (70.8%) were hospitalized and 33 (29.2%) were walk in patients. E. coli was the dominant uro-pathogen 77 (68.1%) followed by Staphylococcus aureus 13 (11.5%), Proteus spp. 9(8.0%), Pseudomonas spp. 6 (5.3%), Klebsiella spp. 4(3.5%), and methicillin resistant Staphylococcus aureus 4 (3.5%). Antibiotic susceptibility test was performed by disc diffusion method according to clinical laboratories standard institute (CLSI). Bacterial isolates showed resistance to ampicillin (72.0%), ciprofloxacin (53.1%), norfloxacin (51.3%) and trimethoprim–sulfamethaxozole (53.1%). Bacterial spp. resistant to other antibiotics was also prevalent. Meropenem was the most effective antibiotic against all the bacterial isolates. In conclusion, high incidence of single and multiple antibiotic resistant bacterial strains is matter of enormous concern. Meropenem was the drug of choice to control urinary tract infections.
Urinary tract infections (UTIs) represent one of the most common diseases encountered in medical practice today (Rashedmarandi et al., 2008). Worldwide 150 million per annum people suffer from urinary tract infections (Stamm and Norrby, 2001). The infections (UTI) are among the most frequent bacterial infections encountered both in the outpatient units and in nosocomial infections. Urinary infections are frequently caused by Enterobacteriaceae (Gales et al., 2000; Akram et al., 2007). Females are more prone to urinary tract infections because of the shortness of the urethra and its closeness to anus which facilitate entrance of fecal flora to urinary tract (Stamm and Norrby, 2001; Ribeiro et al., 2002). The main symptoms of UTI include urgency, increased frequency, pain on urination and a foul odour of urine. The infections are most frequently initiated by an inflammation of the urethra, or urethritis. Among Enterobacteriaceae, E. coli accounts for 75 to 90 percent urinary tract infections (Stamm and Norrby, 2001). E. coli remain the predominant uro-pathogen followed by S. saprophyticus, K. pneumonia, Enterobacter, Proteus spp. and Enterococcus spp. (Garofalo et al., 2007; Raz et al., 2005; Lavanya and Jogalakshmi, 2002; Honkinen et al., 1999; Mohanty et al., 2003; Taneja et al., 2010).
Different bacterial species of urinary tract infections are showing resistant not only to conventional antibiotics but also to new more potent antibiotics (Taneja et al., 2010). This pattern of susceptibility to antibiotics has resulted in increase resistance to commonly used antibiotics over the last decade (Magalit et al., 2004).
In many parts of Khyber Pukhtunkhwa (KPK), lack of facilities for urine culture and antimicrobial susceptibility testing has to improper diagnosis and irrational antibiotic treatment (e.g. self–medication) (Shafiq et al., 2013). The present study is therefore designed to isolate and identify bacterial causes of UTIs and to determine their susceptibility to antibiotics.
A total of two hundred urine samples were collected from the walk-in and hospitalized patients in a tertiary hospital at Peshawar, Pakistan. The samples were processed for urinalysis and culturing after labeling each sample. If delay was to be suspected, boric acid was used (0.1g/10mL of urine) for preservation to prevent multiplication of bacteria. Uncentrifuged urine was analyzed under a microscope and the presence of WBCs more than normal was considered susceptible for UTIs.
Aseptically collected samples were placed on suitable culture medium such as cysteine lactose electrolyte deficient (CLED) agar (Oxoid, UK), Blood agar (Oxoid, UK) and MacConkey’s agar (Oxoid, UK). Each plate was examined for colony count and etiological agent after 18–24 hours of incubation at 37oC. Isolates from positive samples were identified based upon standard laboratory procedures including, morphological characteristics, Gram’s stain, rapid tests (catalase, oxidase, coagulase, bile solubility), and biochemical tests including indole, methyl red, Voges–Proskauer and citrate (IMViC), triple sugar iron (TSI), oxidation/fermentation (O/F), urease and nitrate reduction (Harley and Prescott, 2002).
Antibiotic susceptibility test were performed by CLSI recommended modified Kirby–Bauer disc diffusion method on Mueller–Hinton agar with commercial antibiotic discs (Oxoid Ltd, UK) (CLSI, 2006). Isolates showing an intermediate level of susceptibility were classified as resistant. Antibiotic concentrations used to determine antibiotic susceptibility for bacterial pathogens were: ampicllin (25μg), ciprofloxacin (5μg), nitrofurantoin (300μg), norfloxacin (10μg), Chloramphenicol (30μg), meropenem (10μg), tygacil (15μg), cefazolin (30μg), vancomycin (30μg), methicillin (10μg), Tazocin (30μg), trimethoprim / sulfamethaxozole (1.25μg) and fusidic acid (10μg). As reference strains Staphylococcus aureus (ATCC 25923) and Escherichia coli (ATCC 25922) were used as controls for Gram-positive and Gram-negative bacteria, respectively.
Results about the prevailing pathogens from outdoor and admitted patients are presented in the Table 1. Out of these, 113 were positive for bacterial infection (33 from walk-in patients and 80 from hospitalized patients). E. coli, the predominant pathogen, was more in admitted patients 55 (71.4%) as compared to walk-in patients 22 (28.6%). Staphylococcus aurous in admitted as well as outdoor patients were 8 (61.5%) and 5 (38.5%), respectively. Methicillin resistant strains of Staphylococcus aurous were recovered from admitted patients. Pseudomonas aeruginosa was 5 (83.3 %) in admitted patients and 1 (11.11%) in out-patients. Proteus mirabilis and Klebsiella spp. were 5 (55.6%) and 3 (75%) in admitted patients and were 4 (44.4%) and 1 (25%) in walk-in patients, respectively.

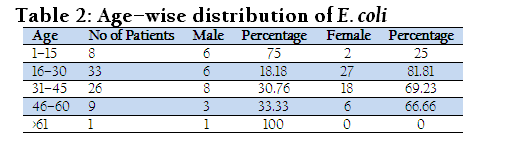
Distribution of UTI patients with respect to medico- demographic characteristic (age 1–15, 16–30, 31–45, 46–60, >61years) is presented in Table 2. Among the total 113 patients, ten (8 male and 2 female) were in the range of 1–15 years of age, thirty (6 male and 24 female) in range of 16–30 years of age, 26 (8 male and 18 female) in range of 31–45 years of age, 3 (3 female) were in range of 46–60 years of age and one female above 60 years of age was found positive. It showed that women were more prone to urinary tract infection in these ages.
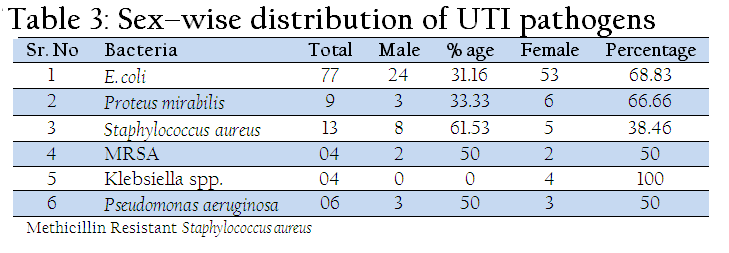
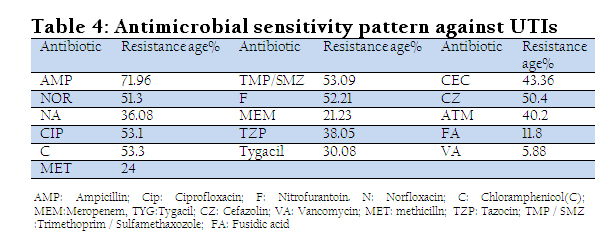
Sex wise distribution of bacterial pathogens of UTI patients is shown in Table 3. Among 113 patients, E. coli was isolated from 24 (31.2%) male and 53 (68.8%) females. Staphylococcus aurous was isolated from 8 (61.5%) male and 5 (38.46%) female. However, four methicillin resistant strains of Staphylococcus aurous were also isolated from 2 (50%) male and 2 (50%) female patients. Proteus mirabilis was recovered from 3 male and 6 female patients. Four Klebsiella and six Pseudomonas aeruginosa were also isolated from UTI patients. Antimicrobial sensitivity pattern of bacterial pathogens isolated from UTIs patients is shown in Table 4. Among bacterial pathogens, 72% isolates were resistant ampicillin, 53% were resistant to ciprofloxacin, 51.3% to norfloxacin, 53.1% to tmp/smz, 52.2% to nitrofurontoin, 40.2% to aztreonam, 53.3% to chlorophenicol, 43.4 % to cefaclor, 50.4% to cefazolin,38% to tazocin, 30.1% to tygacil, 21.2% to meropenem, 36.1% to nalidix acid, 5.9% to fusidic acid, 24% to methicillin and 5.9% to vancomycin, respectively. Four Staphylococcus aurous species were resistant to methicillin and 13 were sensitive to vancomycin and fusidic acid.
Urinary tract infection in human beings is common problem all over the world (Gupta, 2002). Our study showed that Enterobacteriaceae are predominant causative organisms for UTI, followed by Gram–positive cocci, a finding consistent with the results of Pankaj (2012). In present study urine specimens were collected from 200 suspected UTI patients, out of which 113 (56.6%) were positive and 87(43.5%) were negative. Acharya et al. (2011) conducted similar kind of study by collecting 950 samples. Out of these 237 (24.94%) samples grew potential pathogens causing UTI and 713(75.05) were negative.
It was observed that UTI was more in females than male. This is in congurence with Bashir et al. (2008) .They analyzed 109 positive samples in which 36 samples were in male and 73 were in females. UTIs were mainly found in females, the reason might be the shortness of the urethra and its closeness to anus which facilitate entrance of fecal micro–flora to urinary tract. In our study E. coli was more in hospitalized patients 55(71.42%) as compared to walk-in patients 22 (28.57 %). Naeem et al. (2010) studied two groups, outpatient Group I and admitted patients group II in which Escherichia coli was the most common isolate in both groups (60% and 53% in Group I and II respectively). Further, the findings are in correlation with Pankaj et al. (2012) who did describe Escherichia coli the most prevalent organism (81.3%, 178 isolates). With respect to Pseudomonas, our findings are in correlation with the other study in which Pseudomonas spp. was (5.17%) (7.3%), (7%) found to be the causative agent of UTIs, respectively (Ojo and Anibijuwon, 2010; Bashir et al., 2008; Naeem et al., 2010).
In the present study, the incidence of proteus mirabilis was also observed in admitted as well as walk-in patients which is similar to observations made by Ojo and Anibijuwon (2010). Among gram negative bacilli, isolation of klebsiella pneumonia is in agreement with Manikandan et al. (2011) who reported 15.8% incidence of Klebsiella pneumonia among uro-pathogens. Likewise, Mashouf et al. (2009) also reported 10.2% incidence of Klebsiella pneumonia. Considering isolation of methicilline resistant Staphylococcus aureus, the results of the present study are comparable with Mashouf et al. (2009) who reported the incidence of methicillin resistant staphylococcus and staphylococcus aureus in UTI.
With respect to antibiotic susceptibility against a wide range of antibiotics, the results are in agreement with previous observations made by Naeem et al. (2010). Bacterial isolates resistance to two groups named outpatient Group I and admitted patients group II was; amoxycillin, amoxycillin/clavulanate (55% and 24%), Ciprofloxacin (63% and 24%), Levofloxacin (73% and 43%), cefixime, cefotaxime (70% and 38%), ceftriaxone (75% and 37%), cefoperazone/sulbactum (93% and 76%), amikacin, imipenem (95% and 86%) and pipracillin/tazobactum (95% and 86%). Similarly, in another study conducted by Mowla et al. (2011), 92% bacterial strains were resistant to ampicillin (n = 33), 52% of the isolates (n = 19) were resistant to sulfamethoxazole–trimethoprim, 50% (n = 18) to tetracycline, 25% (n = 9) to chloramphenicol, 50% against azithromycin, 8.33% (n = 3) isolates showed resistance against to mecellinum. Among the strains, 72% were resistant to nalidixic acid (n = 26) and 50% (n = 18) were resistant to ciprofloxacin.
Our study concludes that E. coli is one of the important causative agents of urinary tract infection especially in females. High incidence of single and multiple antibiotic resistant bacterial strains is matter of enormous concern. Meropenem was the drug of choice to control urinary tract infections.
REFERENCES
Acharya A, Gautam R and Subedee L (2011). Uropathogens and their antimicrobial susceptibility pattern in Bharatpur, Nepal. Nepal Med. Coll. J. 13: 30–33.
PMid:21991698
Akram M, Shahid M and Khan A (2007). Etiology and antibiotic resistance patterns of community–acquired urinary tract infections in JNMC Hospital Aligarh, India. Annals. Clin. Microbiol. and Antimicrobiol. 6:4.
http://dx.doi.org/10.1186/1476-0711-6-4
PMid:17378940 PMCid:PMC1852324
Bashir MF, Qazi JI, Ahmad N and Riaz S (2008). Diversity of urinary tract pathogens and drug resistant isolates of Escherichia coli in different age and gender groups of Pakistanis. Tropical J. Pharm. Res. 7: 1025–1031.
http://dx.doi.org/10.4314/tjpr.v7i3.14687
Clinical and Laboratory Standards Institute (CLSI) (2006). Performance standards for antimicrobial susceptibility testing. Sixteenth informational supplement document M100–S16 Wayne, PA: Clinical and Laboratory Standards Institute.
Gales CA, Jones RN, Gordon KA, Sader, HS, Wilke, WW Beach, ML Pfaller, MA Doern, GV and the SENTRY Study Group (Latin America) (2000). Activity and spectrum of 22 antimicrobial agents tested against urinary tract infection pathogens in hospitalized patients in Latin America: report from the second year of the SENTRY Antimicrobial Surveillance Program. J. Antimicrob. Chemother. 45: 295–303.
http://dx.doi.org/10.1093/jac/45.3.295
PMid:10702547
Garofalo CK, Hootan TM, SM Martin, Stamm WE, Palmermo, JJ Gordon JI, and Hultgren SJ (2007). E. coli from urine of patients with urinary tract infections is competent for intracelluer bacterial community formation. Infect. Immun. 75: 52–60.
http://dx.doi.org/10.1128/IAI.01123-06
PMid:17074856 PMCid:PMC1828379
Gupta K (2002). Addressing antibiotic resistance. Am. J. Med. 113: S29–S34.
http://dx.doi.org/10.1016/S0002-9343(02)01057-4
Harley JP, Prescott LM (2002). Laboratory exercises in microbiology. 5 edition. Mc–Graw–Hill Publishers; 37–237.
Honkinen O, Lehtonen O, Ruvskunen O, Heovinen P and Mertsola J (1999). Cohat study of bacterial: Species causing urinary tract infections in children. BMJ. 318: 770–771.
http://dx.doi.org/10.1136/bmj.318.7186.770
PMid:10082700 PMCid:PMC27791
Lavanya SV and Jogalakshmi D (2002). Asympotatic bacteriuria in antenatal woman. The new Eng. J. Med. 20: 105–106.
Magalit SL, Gler MTS and Tupasi TE (2004). Increasing antimicrobial resistance patterns of community and nosocomial uropathogens in Makati Medical Center. Phil. J. Microbiol. Infect. Dis. 33: 143–148.
Manikandan S, Ganisapandian S, Manoj S and Kumuraguru AK (2011). Emerging of multidrug resistance human pathogens from urinary tract infections. Curr. Res. Bacteriol. 4: 9–15.
http://dx.doi.org/10.3923/crb.2011.9.15
Mohanty S, Kapil A, Das BK and Dhawan B (2003). Antimicrobial resistance profile of nosocomial uropathogens in a teritiary care hospital. Ind. J. Med. Res. 57: 148–154.
Mashouf RY, Babalhavaeji H and Yousef J (2009). Urinary tract infections: Bacteriology and antibiotic resistance patterns. Ind. Pediatrics. 46(7): 617–620.
Mowla R, Imam AH, Asaduzzaman M, Nasrin N, Raihan, SH and Chowdhury AKA (2011). Emergence of Multidrug Resistant Extended–Spectrum β–Lactamase Producing Eshcherichia coli Associated With Urinary Tract Infections in Bangladesh. J. Basic and Clin. Pharm. 3: 225–228.
Naeem M, Khan M and Qazi SM (2010). Antibiotic susceptibility pattern of bacterial pathogens causing urinary tract infection in a tertiary care hospital. Ann. Pak. Inst. Med. Sci. 6: 214–218.
Ojo OO and Anibijuwon II (2010). Urinary tract infection among female students residing in the campus of the University of Ado Ekiti, Nigeria. Afr. J. Microbiol. Res. 4: 1195–1198.
Pankaj B, Sanjiv N, Bishnu P, Marasini, Kashi RG, Binod L and Basudha S (2012). High prevalence of multidrug resistance in bacterial uropathogens from Kathmandu, Nepal. BMC Res. Notes. 5:38.
http://dx.doi.org/10.1186/1756-0500-5-38
PMid:22260454 PMCid:PMC3296586
Rashedmarandi F, Rahnamaye FM, Saremi M and Sabourian R (2008). A survey on urinary pathogens and their antimicrobial susceptibility among patients with significant bacteriuria. Iran. J. Patho. 4: 191–196.
Raz R, Colondner R and Kunin CM (2005). Who are you– Staphylococcus saprophyticus? Clin. Infect. Dis. 40: 896–897.
http://dx.doi.org/10.1086/428353
PMid:15736028
Ribeiro R, Rossi MP, Guidi HG, and Pinotti JA (2002). Urinary tract ifection in woman. Int. Urogynecol. J. Pelvic floor dysfunct. 13: 198–203.
http://dx.doi.org/10.1007/s192-002-8353-x
http://dx.doi.org/10.1007/s192-002-8352-0
PMid:12140718
Shafiq A, Ayaz A, Ihteram U, Nadia N, Ammar A and Nawab A (2013). Bacteriological and biochemical evaluation of the springs water of district Buner, Khyber Pakhtunkhwa, Pakistan. Int. J. Adv. Res. Tech. 2: 452–460.
Stamm WE and Norrby SR (2001). Urinary tract infections: disease panorama and challenges. J. Infect. Dis. 183: S1–S4.
http://dx.doi.org/10.1086/318850
PMid:11171002
Taneja N, Chatterjee SS, Singh M, Singh S and Sharma M (2010). Pediatric urinary tract infections in a tertiary care center from northern India. Ind. J. Med. Res. 131(1): 101–105.
PMid:20167982



