Research Journal for Veterinary Practitioners
Case Report
Research Journal for Veterinary Practitioners 2 (5): 78 – 81Evaluation of Patho-morphological Changes Associated with a Firearm Injury in Terms of Wound Ballistic in a Dog
Mehmet Eray Alcigir*, Sevil Atalay Vural, Gunay Alcigir
-
Ankara University, Faculty of Veterinary Medicine, Department of Pathology, 06110, Diskapi, Ankara/Turkey
*Corresponding author:erayalcigir@gmail.com; ealcigir@ankara.edu.tr
ARTICLE CITATION:
Alcigir ME, Vural SA, Alcigir G (2014). Evaluation of patho-morphological changes associated with a firearm injury in terms of wound ballistic in a dog. Res. J. Vet. Pract. 2 (5): 78 – 81.
Received: 2014–04–03, Revised: 2014–04–28, Accepted: 2014–05–01
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.rjvp/2014/2.5.78.81
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
In this case report, the morphological findings associated with a firearm injury was examined within the context of wound ballistics observed during the necropsy of an 11 month - old mixed breed female dog. Initially, it was submitted to Department of Pathology, Ankara University, Turkey with the complaint that she had been bitten and killed in a fight. It was completely understood that she had been killed with firearm. It was evaluated and tried to detect the type of gun, used in firing, the entrance angle and location to the body of the bullet, mean distance between gun and body, followed course in the body after firing, damages caused in organs. Histopathologically, lesions in affected tissues and organs caused by bullet were evaluated. It was aimed to draw attention to the forensic pathology of these types of events and injuries that are occasionally encountered in animals.
Accidental or deliberate shooting of domestic and wild mammals and birds is a frequent occurrence, and such shootings often result in death (Aksoy et al., 2013). Injuries are generally caused by bullets or pellets shot from handguns, hunting rifles or shotguns (Kraus, 1992; Aksoy et al., 2013). Handgun injuries are generally encountered in cities, while rifle, shotgun and double - barreled rifle injuries are usually encountered in rural areas (Kraus, 1992; Merck et al., 2007). These types of injuries are sometimes associated with other forms of traumatic injury, and may also be accompanied by various complications such as respiratory distress, lethargy, limping, pneumo - thorax, internal hemorrhage and bone fractures. Death is generally inevitable in cases with severe injuries, or when emergency treatment is not provided. In cases with delayed treatment, tissue and organ necrosis along with other forms of severe damage or secondary infections become prominent and threaten survival; such circumstances often result in the death of the animal.
Ballistics is a field of science investigating the motion, flight and effects of projectiles shot from weapons, such as pellets, bullets, cannonballs and arrows. Wound ballistics focuses on how these projectiles cause physical injury, move through tissues, and lead to various signs/symptoms and complications. Discussions on ballistics often exclusively focus on weapons and the projectiles fired from these weapons; as a result, wound ballistics, which encompasses the effects of these weapons and projectiles, is often overlooked (Munro and Munro, 2008). In this case, we identified firearm injury in a dog brought to the Ankara University, Department of Veterinary Pathology with suspicion of having been bit and killed during a fight, and performed ballistic examinations of the injury; in this context, we drew attention to the forensic pathology of these types of events and injuries that are occasionally encountered in animals.
The dog in question was an 11 month - old female and mixed breed dog. She was kept at a dog shelter, and had not displayed any signs or symptoms of disease until her death. She was found dead with what appeared to be a slight injury, resembling an injury caused from a bite; she had no other wounds or signs on her body. Before she was brought to us, it was assumed that this injury was caused from a fight with the other dogs at the shelter. In this context, we were requested elucidate the cause of death of this case.
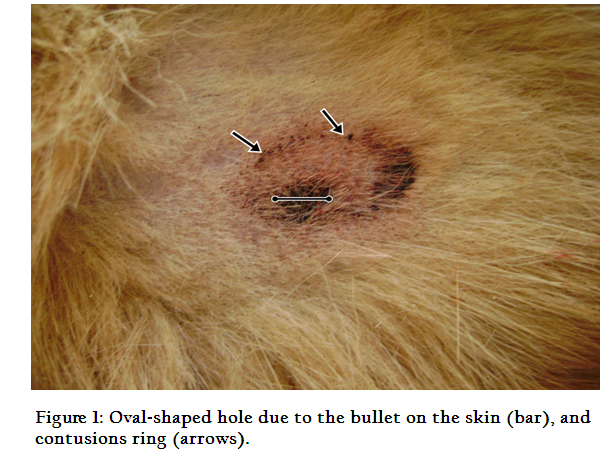
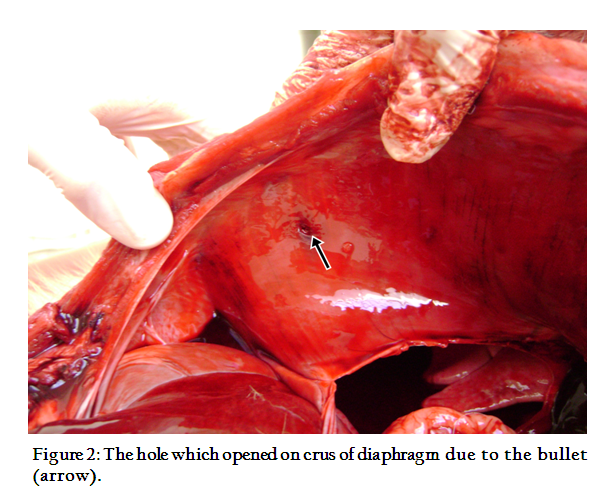
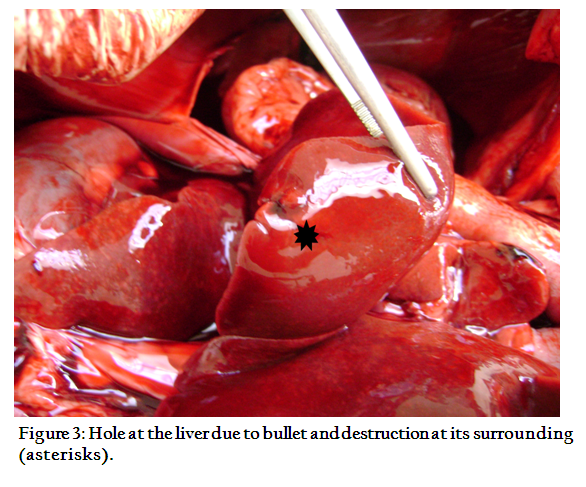
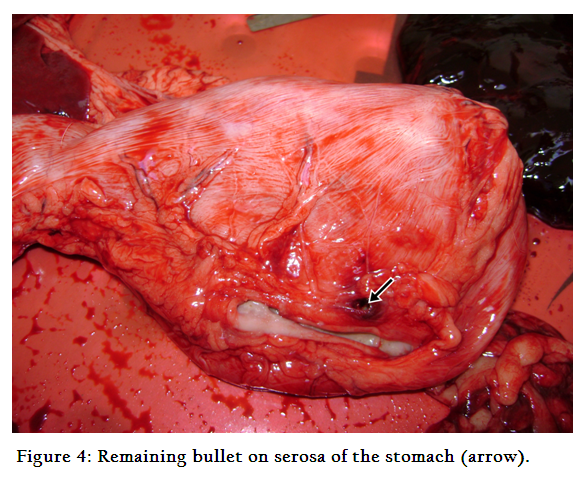
Necropsy examination of the animal revealed that she was well - fed, and that rigor mortis had set in her head, neck and extremities. Her blood had largely coagulated, and her conjunctiva and mouth mucosa had become hyperemic. On the upper one - third of her right thorax, in the area corresponding to the intercostal space between the 3rd and 4th ribs, a disruption of skin integrity was observed. This disruption was associated with a 0.5 cm diameter oval - shaped wound with a regular contour and bleeding in its surroundings. It appeared to have been caused by a piercing object (Figure 1). When the skin was peeled away, ecchymotic bleeding in the muscles beneath the skin of this area, and a perforation advancing from this point into the body cavity were observed. Approximately 10 - 15 ml blood of partially coagulated and omentum was identified in the abdominal cavity, and a certain amount of blood clots were observed on the liver. Another perforation with a diameter of approximately 0.5 cm was observed on the right crus of diaphragm (Figure 2). The liver was swollen, and blood seeped from the cut. On the surface of the lobus caudatus, the tissue integrity was disrupted over an area of a few centimeters (Figure 3). Within the cardial region of the stomach, a small and irregularly - shaped bullet the size of a hazelnut was identified between the serosa and the muscle layer.
In this region, only the tissue surrounding the bullet showed slight bleeding and a dark red color (Figure 4). In the cranial part of the duodenum, areas with bleeding were observed on the serosa and the right lobe of the pancreas. In addition, tympany was observed in certain locations of the small intestines. The spleen was swollen, and its cut surface was bloody. Hyperemia was observed in the kidneys, while hyperemic and emphysematous areas were observed in the lungs. Small amounts of coagulated blood were present on the heart ventricles, while distended blood vessels and edema were observed in the brain.
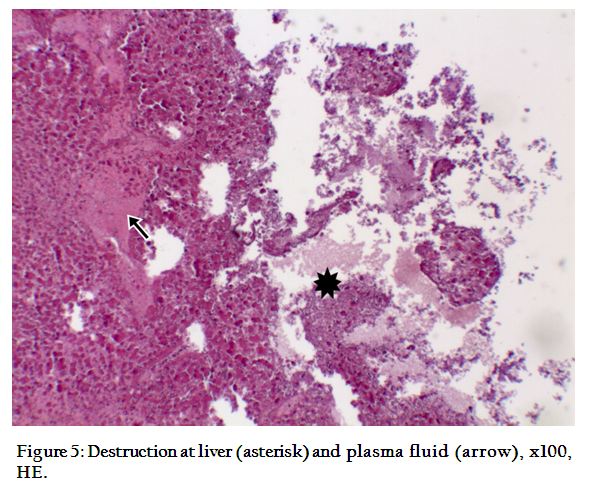
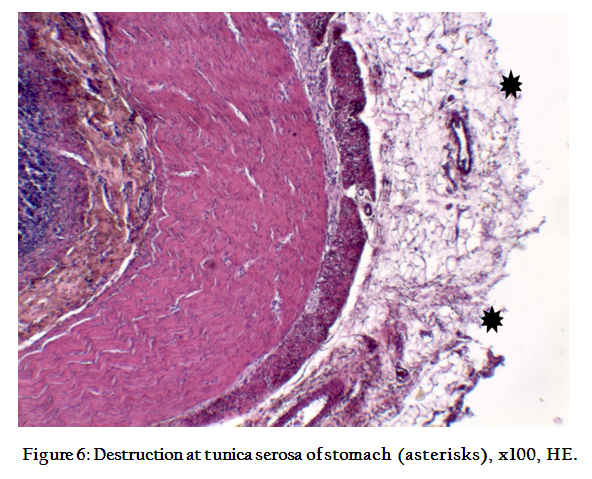
Histopathological evaluation of tissue samples fixed in formalin and stained according to the hematoxylin eosin (HE) method revealed that the bullet had disrupted tissue integrity, ruptured cells and caused bleeding in the regions it passed through. Aside from the region of the stomach where the bullet was found and the surrounding bleedings, no significant tissue disruption was identified. In the liver, the order and organization of the Remak cords was disrupted, and the epitheliums in certain bile ducts were displaced. It was observed that the cytoplasm of hepatocytes in a wide area of the lobus caudatus had acquired an eosinophilic appearance, and that their nuclei were stained pale or had debris. In addition to the intact and broken down erythrocytes in the area, plasma fluid was also observed (Figure 5). The acini of the pancreas were filled with eosinophilic epithelial cells without nuclei. It was also attended that there was destruction in a large area of tunica serosa of stomach (Figure 6). Bleeding was observed in certain areas of the small intestine’s subserosa.
In firearm injuries, part of the kinetic energy of the bullet (KE = bullet mass x bullet speed 2/2) is converted into heat and sound, while part of this energy is converted into mechanical energy; both of these contribute to the damage that occurs in the tissues the bullet passes through, and in the regions surroundings these tissues (Pavletic, 2006; Munro and Munro, 2008). The most important cause of injury in tissues is mechanical and heat energy. Although the nature of an injury depends on the weapon that was used, as well as the speed of the bullet and the distance and angle of the shot, the lesions that result from bullets are all standard. Such lesions involve an entry point where the bullet enters the body, the bullet’s path across the body known as the trajectory, and a exit point that may not always be present (Barach et al., 1986; Kraus, 1992; Merck, 2007; Munro and Munro, 2008; Aksoy et al., 2013). In the current case, the bullet entered the body from the right side of the thorax, pierced the crus of diaphragm through the intercostal space between the 3rd and 4th ribs, passed into the abdominal cavity, scraped the caudate lobe of the liver, and ended its trajectory in the cardia region of the stomach; however, there was no exit point.
The exit point is not indicative of firearm injury’s characteristics. It consists of a tear that is larger than the entry point, and skin flaps that are curved outwards. The morphological characteristics of the entry point, on the other hand, provide clues regarding the distance of the shot, the direction and type of the bullet, and the location of the injured. In shots taken from long distances, the diameter of the entry point is smaller than that of the bullet. A bullet entering the body at a right angle will have a round - shaped entry point, while a bullet entering the body at a more inclined, narrower angle will have an oval - shaped entry point. If a bullet follows an irregular and wobbling course across the air, its entry point will be undulated. The characteristics of the entry point also vary according to the distance of the weapon from the body. Shots in which the barrel presses against the body or are made from a distance of 0 to 3 cm are known as contact shots. The distance of close shots is 35 - 45 cm for handguns and 100 - 150 cm for rifles. Distant shots refer to shots made from longer ranges. In close shots, black - brown contusion rings caused by the conversion of the bullet’s energy into heat and the friction of the bullet are observed at the injury site. Depending on the proximity of the shot, tattoo - like marks consisting of gunpowder remains may also form. In addition, an erasure line between the entry point and the contusion ring may be formed by the oils, rust and dirt covering the bullet. In contact shots, a stamp - like mark of the barrel is formed on the skin due to the vacuum associated with the gases exiting the barrel at the time of the shot (Barach, 1986; Uzar et al., 1998; Dudu and Arman, 2003; Pavletic, 2006; Munro, 2008). Distant shots do not provide such information. As low caliber handgun bullets shot from a distances greater than 40 - 60 cm often leave a small hole at the entry point, these types of injuries are often mistaken for other traumatic injuries formed by tissue perforation; the actual cause of these injuries are elucidated by radiological examination or necropsy (Kraus et al., 1992). The description of the injury on the skin as a bite injury in the initial anamnesis was considered to be associated with this particular characteristic of low caliber bullets. The oval shape of the entry point and the absence of any others findings in the entry point area indicated that the shot was made from a distance, and that bullet had reached the skin from the right side at a narrow angle of 30 - 45 degrees. The trajectory of the bullet inside the body is an important clue for determining the direction of the shot, even though interpreting such information may sometimes prove to be difficult. The position of the shooter and the injured, as well as changes in trajectory due to impact with harder tissues such as bones, are factors that affect the bullet trajectory (Uzar et al., 1998; Pavletic, 2006; Munro and Munro, 2008; Aksoy et al., 2013). In our case, the bullet had not changed its trajectory since it mostly passed through soft tissues. It entered the right thoracic cavity, passed through the abdominal cavity, crossed the edged on the livers, and ended its trajectory in the cardia of the stomach. As such, it was considered that the shot was made while the animal was in a sitting position, or in a leaned position close to the shooter. Alternatively, the shot may have also been made from the right side and at a perpendicular angle, from the craniodorsal to the caudoventral of the animal.
In thorax injuries, bullets that pierce the thorax and have large exit points can lead to sudden death due to pneumothorax. Injuries with small entry points, however, generally do not result in such deaths (Dudu and Arman, 2003; Pavletic, 2006; Munro and Munro, 2008; Aksoy et al., 2013). The fact that our case’s injury consisted only of an entry point as well as the fact that the bullet’s trajectory passed through the abdominal cavity precluded the possibility of such a complication. Another factor that might contribute to sudden death in these types of injuries is hemorrhagic anemia. However, the possibility of a sudden death caused by blood loss was also excluded due to the fact that blood and blood clots indicative of internal bleeding were found only in the abdominal cavity, and also due to the fact that, contrary to findings indicative of hemorrhagic anemia, the tissues and organs of our case were hyperemic.
The lack of severe bleeding in our case was associated with limited damage caused by the bullet due to its trajectory across soft tissues, and also with the bullet’s loss of energy and inability to exit the body. This situation was considered to be indicative of a shot made from long range with a low caliber bullet (Barach et al., 1986; Cooper and Ryan, 1990). This is because the energy of a bullet travelling through the body is well absorbed by hard tissues such as bones, and also by tissues rich in elastic fibers such as muscles. For this reason, less damage occurs in these types of tissues. On the other hand, parenchymatous organs with rich blood supplies such as the spleen, liver and kidneys may be indirectly affected and damaged from the pressure and shock waves of the bullet, even when they are not subject to the bullet's mechanical effects. This is because fluids such as blood are good conductors for shock waves (Cooper and Ryan, 1990). The findings we observed in the pancreas, the intestinal serosa and partly in the liver (all of which were outside the trajectory of the bullet), demonstrated that the bullet had damaged surrounding tissues with its shock waves. The presence of coagulated blood in the heart ventricles, as well as the presence of hyperemia in various tissues and organs, indicated that late complications caused by an impairment of blood circulation might have ultimately lead to our case’s death.
We considered that the animal was killed by a short - barreled weapon shot from long range, and that the bullet penetrated towards the thoracic wall from the right side at a perpendicular angle, and moved downwards following a trajectory towards the abdominal cavity; the bullet came to a stop in the abdominal cavity after its energy was absorbed by the surrounding tissues. Death was not caused suddenly by complications such as pneumothorax or blood loss directly associated with the effects of the bullet. Instead, death resulted from late complications associated with damage and injury caused by pressure waves that formed within organs and tissues on the bullet trajectory. Thus, we considered that the animal continued to live for a certain time after being shot and before succumbing to its wound. In light of this information, we believe that our case will serve as an example for veterinary forensic pathology.
REFERENCES
Aksoy E, Çoltu A, Ege B, Günaydın G, Inanıcı MA, Karali H, Karagöz M, Ötker C, Yemisçigil A (2013). Adli Travmatoloji. [http://www.ttb.org.tr/eweb/adli/4.html], Access date: 15.01.2013.
Barach E, Tomlanovich M, Nowak R (1986). Ballistics: A pathophysiologic examination of the wounding mechanisms of firearms. J. Trauma Acute Care Surg. 26: 225 - 35.
http://dx.doi.org/10.1097/00005373-198604000-00012
http://dx.doi.org/10.1097/00005373-198603000-00003
Cooper GJ, Ryan JM (1990). Interaction of penetrating missiles with tissues. Braz. J. Surg. 77: 606 - 10.
http://dx.doi.org/10.1002/bjs.1800770604
PMid:2200549
Dudu C, Arman B (2003). Toraks travmalarının geç komplikasyonları. Bull. Thoracic Surg. 360 - 385.
Kraus KH (1992). Acute Management of Open Fractures, Including Gunshot, Shearing and Degloving Wounds. In: R.W. Kirk and D.J. Bonagura (eds), Kirk's Current Veterinary Therapy XI: Small Animal Practice, WB Saunders, Philadelphia, USA, 154 - 158.
Merck MD (2007). Patterns of Non - accidental Injury: Gunshot Wounds. In: M.D.Merck (ed), Veterinary Forensics Animal Cruelty Investigations, Blackwell Publishing, Iowa, USA, 131 - 153.
Munro R, Munro HMC (2008). Firearms Injuries. In: R. Munro and H.M.C. Munro (eds), Animal Abuse and Unlawful Killing Forensic Veterinary Pathology, Saunders Elsevier, Edinburg, UK, 55 - 64.
http://dx.doi.org/10.1016/B978-0-7020-2878-6.50017-9
Pavletic MM (2006). Managing gunshot wounds in small animals. Vet. Tech. 27(1): 36 - 44.
Uzar AI, Gulec B, Kayahan C, Ozer MT, Oner K, Alpaslan F (1998). Yara balistigi I. kalıcı ve geçici kavite etkileri. Ulus Travm. Derg. 4: 225 - 229.



