Advances in Animal and Veterinary Sciences
Research Article
Advances in Animal and Veterinary Sciences. 1 (2S): 29 – 32Special Issue–2 (Clinical Veterinary Practice– Trends)
Effect of Butorphanol and Buprenorphine on Inhalant Sparing and Gas Concentrations during Low Flow Isoflurane Anaesthesia in Cattle
S.Senthil Kumar*, N. Rajendran, S. Dharmaceelan, S. Kathirvel, M. Subramanian, P. Selvaraj
-
Department of Veterinary Surgery and Radiology, Veterinary College and Research Institute (TANUVAS), Namakkal, Tamil Nadu – 637 002, India.
*Corresponding author:ssenthilvet@gmail.com
ARTICLE CITATION:
Kumar SS, Rajendran N, Dharmaceelan S, Kathirvel S, Subramanian M and Selvaraj P (2013). Effect of butorphanol and buprenorphine on inhalant sparing and gas concentrations during low flow isoflurane anaesthesia in cattle. Adv. Anim. Vet. Sci. 1 (2S): 29 – 32.
Received: 2013–12–18, Revised: 2013–12–28, Accepted: 2013–12–31
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/4/199/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The purpose of the study was to assess the isoflurane sparing effect of butorphanol and buprenorphine during low flow isoflurane anaesthesia in cattle. The study was conducted in 30 cattle divided into three equal groups. Acepromazine premedication at the dose rate of 0.04 mg/kg i.v. was employed in the animals of all the groups. Butorphanol 0.02 mg/kg i.v. was administered five minutes prior to acepromazine in group II and buprenorphine 0.006 mg/kg i.v. fifteen minutes prior to acepromazine in group III.. In all the groups, guaifenesin 50 mg/kg and ketamine 4 mg/kg were administered intravenously to induce anaesthesia, which was maintained with isoflurane employing rebreathing circle. The end–tidal isoflurane concentration was significantly lower in the groups that received butorphanol or buprenorphine compared to the control group indicating that inclusion of opioids in the anaesthetic protocol had a significant isoflurane sparing effect.
INTRODUCTION
General anaesthesia in cattle may be preferred over other techniques, particularly for complex and prolonged surgical procedures when the technical and anatomical aspects of the surgical procedure warrant absolute control of pain and movement during surgery. Maintenance of anaesthesia with inhalants in ruminants is considered to be superior to injectable techniques. The excessive cardiopulmonary depression caused by deep plane of inhalant anaesthesia can be avoided by inclusion of opioids in the anaesthetic protocol. Pain in cattle is a stressor and elicits a stress response which is very important and has economic concerns because it can cause potential production loss (Bomzon, 2011). Effective management of pain associated with surgery is of paramount importance in preventing stress in cattle. Opioids are well known for their analgesic effects during and after surgery. The use of opioids in the anaesthetic protocol may be of importance, but there is a paucity of literature on the use of opioid analgesics in cattle. Hence, the present study was designed to assess the isoflurane sparing effect of butorphanol/ buprenorphine during low flow isoflurane anaesthesia in cattle.
MATERIALS AND METHODS
The study was conducted in 30 clinical cases of cattle presented to the Large Animal Surgery Unit for right flank laparotomy under general anaesthesia. The animals were randomly divided into three equal groups viz., group I, II and III. The marginal auricular vein was cannulated with an 18GA, 1.77 inch intravenous cannula (BD Venflon™, Becton Dickinson Infusion Therapy AB SE –251 06 Helsingborg, Sweden) to facilitate administration of drugs and fluids during the trial. Acepromazine maleate was administered i.v. at the dose rate of 0.04 mg per kg body weight in all the animals. Butorphanol tartrate (0.02 mg/kg body weight) in group II and buprenorphine hydrochloride (0.006 mg per kg body weight) in group III were administered i.v. 5 and 15 min prior to acepromazine maleate administration, respectively. Five minutes later to acepromazine maleate administration, guaifenesin as a 5 per cent solution in 5 per cent dextrose normal saline was administered at the dose rate of 50 mg per kg body weight i.v. and anaesthesia was induced with ketamine hydrochloride administered intravenously at the dose rate of 4 mg per kg body weight. Oroendotracheal intubation with cuffed Murphy type endotracheal tube was accomplished in all the animals by digital palpation of the larynx employing Gunther’s mouth gag. The endotracheal tube’s cuff was inflated to provide a secure leak–free airway. The correct placement of the endotracheal tube was confirmed by the appearance of capnographic waveforms on the vital sign monitor. The endotracheal tube was connected to the Y piece of the breathing tube through the IRMA airway adaptor of the multigas monitor by a locally fabricated rubber adaptor to maintain and monitor anaesthesia. The large animal anaesthetic machine with ventilator (Mallard Medical Model 8300C®, Redding CA, USA) was used to maintain anaesthesia. An 18 litres capacity ascending bellows of the built–in ventilator of the anaesthetic machine was used as a rebreathing bag during maintenance of anaesthesia. The oxygen flow rate was set at 10 litres per minute for the first 3 min to attain denitrogenation of the anaesthetic circle and also to increase the fraction of inspired–oxygen concentration. The fresh gas flow rate was then reduced to 3 to 5 litres based on the size of the animal. The fresh gas flow rate was adjusted to maintain the bellows of the ventilator at zero marking at the end–expiratory phase. The vapourizer setting was altered during anaesthesia and uniform surgical plane of anaesthesia was maintained. The changes, made on the fresh gas flow rate and vapourizer setting at various times, during maintenance of anaesthesia were recorded. All the experimental trials were conducted at the large animal operating room with ambient temperature maintained at 30ºC. The volume of isoflurane vapour delivered at 30ºC from 1 mL of commercially available isoflurane liquid was calculated employing Avogadro’s principle based on its density and incorporating temperature correction. The Schiller Argus Multigas Truscope® monitor was used to measure the inspired and end–tidal oxygen, carbon dioxide and isoflurane concentration continuously during maintenance of anaesthesia. The average value measured was recorded in all the animals. The isoflurane utilized for maintenance of anaesthesia was calculated based on the fresh gas flow rate employed, total duration of inhalation anaesthesia and the vapourizer setting employed for each animal and the value was equated to 300 kg body weight and 1 h basis for ease of understanding and comparison. The quantity of isoflurane liquid utilized for maintenance of anaesthesia was calculated as mentioned below employing Avogadro’s principle as described by Steffey and Mama (2007). The total duration of anaesthesia (1) in min was estimated from the time of turning on the vapourizer to the time of turning off the vapourizer.
The average fresh gas flow rate (FGF) (mL/kg/min) employed during maintenance of anaesthesia was calculated by the following formula,
Average fresh gas flow rate(mL/kg/min) |
= |
Total FGF employed (L) x 1000 |
|
|
Body weight x Total duration of anaesthesia(1) |
The duration of anaesthesia (2) in min for each vapourizer setting and/or fresh gas flow rate employed was recorded and isoflurane vapour delivered (mL) (3) was calculated by the formula mentioned below.
Formula II
Isoflurane vapour delivered (mL) (3) |
= |
Vapourizer setting (%) X FGF (LPM) X Duration (min) (2) X 10 |
The total isoflurane vapour delivered (mL) (4) for the total duration of anaesthesia (1) was calculated by summing up the isoflurane vapour delivered (3) for each of the FGF and vapourizer setting employed. The total isoflurane vapour value so obtained was equated to 300 kg body weight and 1 h duration basis for statistical comparison as follows,
Formula III
Isoflurane vapour delivered for 300 kg and 1 h basis (mL) (5) |
= |
Total isoflurane vapour delivered (mL) (4) x 300 x 60 |
|
|
Body weight x Duration of maintenance (1) |
The isoflurane liquid utilized (mL) for 300 kg and 1 h basis (6) was calculated from the above value as follows,
Formula IV
Isoflurane liquid utilized (mL) for 300 kg and 1 h basis (6) |
= |
Isoflurane vapour delivered for 300 kg and 1 h basis (mL) (5) |
|
|
201.5 |
The isoflurane sparing effect of butorphanol tartrate and buprenorphine hydrochloride in groups II and III was calculated from the difference in the total liquid isoflurane used in group I. The economics of low flow isoflurane anaesthesia was calculated from the isoflurane liquid utilized (mL) and cost of isoflurane.
The data obtained were analyzed using F–Test for variances and t–test for comparison of means between the groups as described by Snedecor and Cochran (1994) using SPSS®10 software package.
RESULTS
The mean (± SE) fresh gas flow rate (mL per kg per min) employed during low flow isoflurane anaesthesia was 19.28±2.60, 12.52±0.95 and 16.93±2.84 in group I, II and III animals, respectively. Statistical analysis revealed that the fresh gas flow rate employed among groups differed significantly (p<0.01). The fresh gas flow rate employed in group II was the least among the three groups. The mean (± SE) total duration of inhalation anaesthesia (min) was 64.33±14.12, 65.00±14.93 and 83.17±7.12 in group I, II and III animals, respectively. The total duration of inhalation anaesthesia was significantly longer (p<0.01) in group III compared to groups I and II. The total duration of inhalation anaesthesia between groups I and II did not differ significantly. The mean (± SE) equated isoflurane liquid utilized for 300 kg and 1 h basis was 43.85±6.20, 26.00±3.20 and 31.06±5.44 mL in group I, II and III animals, respectively. Statistical analysis revealed a highly significant difference (p<0.01) in the utilization of isoflurane liquid equated for 300 kg and 1 h basis among the three groups. Utilization of isoflurane was comparatively lower in group II followed by group III and group I.
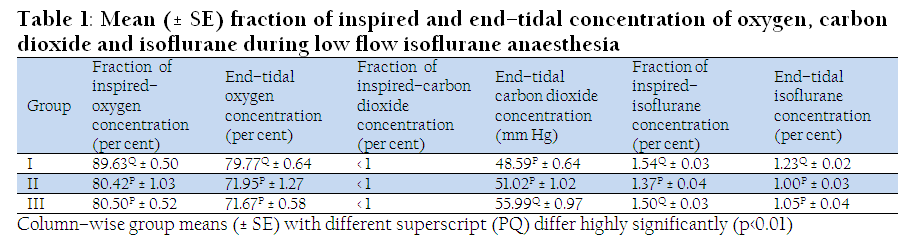
Table 1: Mean (± SE) fraction of inspired and end–tidal concentration of oxygen, carbon dioxide and isoflurane during low flow isoflurane anaesthesia
The fraction of inspired–oxygen concentration in group I was significantly higher compared to group II and III (Table 1). The end–tidal oxygen concentration in group I was significantly higher compared to group II and III. The end–tidal concentration of carbon dioxide was significantly higher in group III compared to group I and II. The tidal volume in group III was significantly higher but the minute volume was significantly lower due to decreased respiratory rate (Table 2). The fraction of inspired–isoflurane concentration in group I was significantly higher than group II and III. The end–tidal isoflurane concentration was significantly lower in group II and III compared to group I.
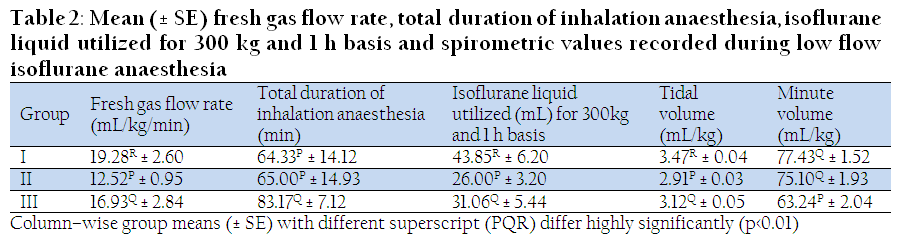
Table 2: Mean (± SE) fresh gas flow rate, total duration of inhalation anaesthesia, isoflurane liquid utilized for 300 kg and 1 h basis and spirometric values recorded during low flow isoflurane anaesthesia
There was 18.70 per cent reduction in minimum alveolar concentration of isoflurane in group II and 14.63 per cent in group III animals. Statistical comparison revealed that butorphanol tartrate and buprenorphine hydrochloride had a significant (p<0.05) isoflurane sparing effect.
There was 40.71 per cent reduction in consumption of isoflurane in group II animals and 29.17 per cent in group III animals (Table 2). The reduction in utilization of isoflurane in group II and III was statistically significant (p<0.05) compared to group I.
The cost of low flow isoflurane anaesthesia for maintenance was calculated from the isoflurane liquid utilized for 300 kg body weight cattle and 1 h duration. The prevailing market rate of commercially supplied isoflurane liquid per mL was estimated to be Rs. 10.00. The cost of low flow isoflurane anaesthesia for maintenance of 1 h duration in cattle weighing 300 kg was Rs.438.50, 260.00 and 310.60 in group I, II and III animals, respectively. There was a significant reduction (p<0.05) in the cost of isoflurane utilized during low flow isoflurane anaesthesia in groups II and III compared to group I animals.
DISCUSSION
The lower fresh gas flow rate employed in groups II and III than group I could be attributed to the decreased inhalant requirement owing to inhalant sparing effect of the opioids included in the anaesthetic protocol. The difference in the duration of anaesthesia among the three groups was due to the difference in the duration to complete the intended surgical interventions.
The isoflurane liquid utilized in groups II and III was significantly lower than that in group I. This could be attributed to the isoflurane sparing effect of opioids, butorphanol tartrate and buprenorphine hydrochloride, included in the anaesthetic protocol.
The fraction of inspired–oxygen concentration in group I was significantly higher compared to group II and III. This could be due to the increased FGF employed in group I. The FGF employed during maintenance of anaesthesia was considered a determining factor to achieve increased fraction of inspired–oxygen concentration. Becker and Casabinaca (2009) reported that oxygenation remained adequate for considerable time despite the presence of hypoventilation when supplemental oxygen was provided. The authors stated that the potential benefit of supplemental oxygen must be weighed against false sense of security provided by the pulse oximetry in the absence of ventilation monitoring. The authors were of the opinion that supplemental oxygen increased the concentration of oxygen in the functional residual capacity and delayed the onset of hypoxaemia when the patient experienced airway obstruction, hypoventilation or apnea. The fraction of inspired–oxygen concentration recorded in the three groups of animals correlated with the FGF employed and this concurs with the findings of Hubbell et al. (2011). The potency of isoflurane permitted the concomitant administration of 100 per cent oxygen to increase the fraction of inspired–oxygen concentration and concurs with the recommendations of Eger (1981). Higher end–tidal oxygen concentration in group I could be attributed to the increased fraction of inspired–oxygen concentration. The higher end–tidal oxygen concentration recorded in all the animals was observed to be beneficial in maintaining normal saturation of peripheral oxygen. Similar observations were recorded by Hubbell et al. (2011).
The fraction of inspired–carbon dioxide concentration was monitored continuously throughout the low flow isoflurane anaesthesia and at all times it was less than one per cent. This indicated that the carbon dioxide removal by the soda lime was effective and performance of the unidirectional valve of the anaesthetic circle was satisfactory. This concurs with the recommendations of Tranquilli et al. (2007). The end–tidal concentration of carbon dioxide was significantly higher in group III compared to group I and II. The tidal volume in group III was significantly higher but the minute volume was significantly lower due to decreased respiratory rate. The significant decrease in the ventilation could be ascribed to the depression of respiratory centre’s response to hypercapnia by buprenorphine resulting in carbon dioxide retention leading to increased end–tidal concentration of carbon dioxide in group III animals. Similar respiratory depression and increased ventilation/perfusion mismatch was reported with use of volatile inhalant anaesthetics (Tranquilli et al. 2007). The depressant effect on respiratory system by opioids and volatile agents were reported to be additive and the results of the present study concurs with Roberts and Kestin (2008).
Higher fraction of inspired–isoflurane concentration in group I than group II and III could be attributed to the higher FGF and vapourizer setting employed in group I. Bilbrough (2006) stated that simple relationship between the vapourizer setting and inspired concentration of inhalant did not exist at very low flow rates when circle breathing system was used. The author concluded that end–tidal inhalant percentage measured could be used to relate the levels of inhalant achieved in the central nervous system. The higher fraction of inspired–isoflurane concentration delivered in all the groups was required to wash out the anaesthetic circuit, to counter balance the depletion of isoflurane in rebreathed gases and to account for loss of anaesthetic in soda lime. Eger (1981) recommended similar protocol to achieve desired end–tidal isoflurane concentration.
The end–tidal isoflurane concentration was significantly lower in group II and III compared to group I indicating that the inclusion of opioids, butorphanol tartrate and buprenorphine hydrochloride in the anaesthetic protocol had produced isoflurane sparing effect. The decreased requirement of end–tidal isoflurane concentration in group II and III could be attributed to the analgesia provided by butorphanol tartrate and buprenorphine hydrochloride. Similar observations were recorded by Doherty et al. (1997). The low blood solubility of isoflurane permitted end–tidal isoflurane concentration to rise rapidly towards the inspired concentration. The alveolar concentration of isoflurane rose to 50 per cent of that inspired in the first 5 to 10 min of anaesthesia and equaled 70 per cent of the inspired concentration after 30 min of anesthesia and concurs with the observations of Eger (1981).
Comparison between groups II and III revealed that butorphanol tartrate had better isoflurane sparing effect. This could be due to the effective analgesia provided by butorphanol tartrate than buprenorphine hydrochloride in cattle. Similar observations were recorded by Doherty et al. (1997) and Thurmon et al. (1996).
The significant reduction in the MAC requirement of isoflurane in groups II and III indicated that the inclusion of butorphanol tartrate and buprenorphine hydrochloride in the anaesthetic protocol had resulted in prominent isoflurane sparing effect. The isoflurane sparing effect caused by the butorphanol tartrate and buprenorphine hydrochloride had resulted in decreased consumption of isoflurane for maintenance of anaesthesia. The decreased consumption of isoflurane for maintenance of anaesthesia signified that the usage of isoflurane, a potent global warming inhalant, was efficient. The efficient usage of potent costly isoflurane inhalant reduced the polluting potential rendering the anaesthetic protocol cost–effective.
The inclusion of the opioids, butorphanol and buprenorphine, in the anaesthetic protocol of cattle was found to have significant inhalant sparing effect rendering the protocol safe and cost–effective.
REFERENCES
Bilbrough G (2006). A Practical guide to capnography. In Pract. 28: 312–319.
http://dx.doi.org/10.1136/inpract.28.6.312
Bomzon A (2011). Pain and Stress in Cattle: A Personal Perspective. Israel J. Vet. Med. 66:12–20.
Doherty TJ, Geiser DR and Rohrbach BW (1997). Effect of acepromazine butorphanol on halothane minimum alveolar concentration in ponies. Equine Vet. J. 29: 374–376.
http://dx.doi.org/10.1111/j.2042-3306.1997.tb03141.x
http://dx.doi.org/10.1111/j.2042-3306.1997.tb03142.x
PMid:9306064
Eger EI II (1981). Isoflurane: A Review. Anesthesiology 55: 559–576.
http://dx.doi.org/10.1097/00000542-198111000-00014
PMid:7027831
Hubbell JAE, Aarnes TK, Bednarski RM, Lerche P and Muir WM (2011). Effect of 50% and maximal inspired oxygen concentrations on respiratory variables in isoflurane–anesthetized horses. BMC Vet. Res. 7: 23. http://www.biomedcentral.com/1746-6148/7/23 Accession date: 22.01.2013.
Roberts F and Kestin A (2008). Respiratory Physiology. Update in Anaesthesia 24: 15–19.
Snedecor GM and Cochran WC (1994). Statistical methods. 9th edn., Oxford and IBM Publishing Company, Mumbai, India.
Steffey EP and Mama KR (2007). Inhalational anesthetics. In: Tranquilli WJ, Thurmon JC and Grimm KA (eds), Lumb and Jones' Veterinary Anesthesia and Analgesia, 4th edn., Blackwell Publishing, Iowa, USA, 355–393.
Thurmon JC, Tranquilli WJ and Benson GJ (1996). Lumb and Jones' Veterinary Anaesthesia. 3rd edn., Williams and Wilkins, Baltimore, USA.
Tranquilli WJ, Thurmon JC and Grimm KA (2007). Lumb and Jones' Veterinary Anesthesia and Analgesia. 4th edn., Blackwell Publishers, Iowa, USA.



