Advances in Animal and Veterinary Sciences
Case Report
Advances in Animal and Veterinary Sciences. 1 (1S): 23 – 28Special issue-1 (Veterinarians approaches for safeguarding animal health and production)
Therapeutic Management of Clinical Bovine Johne’s disease Using Goat Based ‘Indigenous Vaccine’ in Native Hariana Cattle: Case Reports
Shoor Vir Singh1*, Saurabh Gupta1, Pravin Kumar Singh2, Ajay Vir Singh2, Jagdip Singh Sohal3, Naveen Kumar1, Avnish Kumar4, Kundan Kumar Chaubey1, Brajesh Singh1
- Microbiology Laboratory, Animal Health Division, Central Institute for Research on Goats, Makhdoom, PO – Farah, Mathura, Uttar Pradesh, India
- National JALMA Institute for Leprosy and Other Mycobacterial Diseases, Tajganj, Agra, Uttar Pradesh, India
- Canadian Food Inspection Agency, 3400 W Casavant, St. Hyacihthe (QC), Canada– J2S 8E3
- School of Life sciences, Khandari, Agra, Uttar Pradesh, India
*Corresponding author:shoorvir.singh@gmail.com; shoorvir_singh@rediffmail.com
ARTICLE CITATION:
Singh SV, Gupta S, Singh PK, Singh AV, Sohal JS, Kumar N, Kumar A, Chaubey KK and Singh B (2013). Therapeutic Management of Clinical Bovine Johne’s disease Using Goat Based ‘Indigenous Vaccine’ in Native Hariana Cattle: Case Reports. Adv. Anim. Vet. Sci. 1 (1S):23 – 28.
Received: 2013–08–17, Revised: 2013–09–15, Accepted: 2013–09–16
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/4/101/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Study reports therapeutic management of clinical to advance clinical Bovine Johne’s disease in a young male calf and an adult dairy cow of native Hariana breed in Mathura district. Calf (14 months old) suffering from symptoms of clinical bovine Johne’s disease (weakness and stunting without diarrhoea) was negative for MAP infection in fecal microscopy, blood PCR and ELISA, An adult cow (144 months old) a case of advance clinical BJD (suffering from non–treatable diarrhoea for last 3 years and weakness) was positive in ELISA and negative in microscopy and blood PCR tests. After exhausting all possible therapies, both the animals were vaccinated with 2 ml of ‘indigenous vaccine’ made from ‘Indian Bison Type’ biotype of Mycobacterium avium subspecies paratuberculosis (strain S 5) of goat origin, as last option. ‘Indigenous vaccine’ effectively helped in the management of clinical JD in case of calf however immune response was limited and not sufficient in the cow to fully recover from advance clinical JD. The study besides exhibiting therapeutic potential of goat based ‘indigenous vaccine’, also underlined the critical role of nutrition in response to vaccination and in management of chronic infections, just as it hastens or delays the precipitation of disease from sub–clinical to clinical or advance clinical stage. The study also exposed limitation of laboratory tests used for the diagnosis of clinical BJD.
Mycobacterium avium subspecies paratuberculosis (MAP) cause Johne’s disease (JD) in domestic livestock and other animals including primates (Singh et al., 2013a). The disease is endemic in the population of domestic cattle in the country (Sharma et al., 2008; Mishra et al., 2009; Singh et al., 2013a). Though number of dairy animals is highest in the country and is leading milk producer (117 million tonnes) in the world (FAO, 2012) however, per animal productivity is very low. Majority of dairy cattle are in small herds (3 – 5) or as individual animals in milk. Due to high population density of animals there is drastic reduction in grazing and fallow land. There is marked shift in husbandry practices and animals are confinement to either one place or in very limited area, where they are taken daily for grazing or watering. Therefore, in the absence of policy on control of JD and under confined husbandry practices, country is waking up to the new challenge of the chronic infections like JD, since JD has long been considered as the disease of large herds and flocks. In this scenario, JD appears to be major cause of low per animal productivity of the native livestock breeds. This low per animal productivity may be directly correlated with high prevalence of JD in Indian livestock. Low priority to JD is also due to lack of information on incidence of MAP in domestic livestock population of the country. Presently country lacks indigenous, rapid, sensitive and cost–effective diagnostic tests and high cost of imported kits are main reasons for lack of attention on JD. Treatment of disease is both uneconomical and impractical (Harris and Barletta, 2001). Since ‘cow slaughter’ is banned in the country, therefore vaccination is the only alternative for the management of bovine JD infecting cattle. ‘Indigenous vaccine’ developed for the control of disease in goats has also shown promise to treat, manage and control infection of MAP in animals other than goats (Singh et al., 2013b).
In the present case reports, two animals (a young male calf and an adult lactating cow) were vaccinated with ‘indigenous goat based vaccine’ in effort to treat these animals of the clinical bovine Johne’s disease.
An adult dairy cow (14 months old, female) of Hariana breed belonged to a poor and landless farmer of village Begampur, located on the other side of bank of Yamuna river near holy city of Vrindavan in Mathura district of Uttar Pradesh. As per owner this cow had calved >8 times and was still giving 300–500 mL of milk per milking in a day (two times milking/ day) despite suffering from diarrhoea continuously for past three years and has soiled all the wall of the courtyard of his small house. The owner had only this cow as the source of milk for family and was small time contract farmer to earn livelihood and took cow with him for grazing on farm boundaries. For the treatment of his cow, the farmer was taking help of a local NGO (project Balram), run by CDHIFI (Chandi Duke Heffner International Foundation of India) in Vrindavan, Mathura for last >6 months. The cow was treated by veterinary experts of the NGO with antibiotics, antiparasitic (Ivomac injection, Merial, USA), antidiarrhoeal drugs and supportive therapy. However, there was limited response in diarrhoea, till antibiotic tablets lasted. As soon as antibiotics were stopped, there was relapse in diarrhoeal intensity. The nutritional status of cow was low as she depended on 8–10 hr grazing (extensive management) and little supplement with wheat straw and some wheat flour, while at home. Physical condition of cow was indistinguishable to that of ‘advance clinical JD’. However, screening of serum, blood and fecal samples of the cow (provided by CDHIFI) twice before vaccination were negative in fecal microscopy and blood PCR but was positive in ‘indigenous ELISA’ test. The cow was in a stage where it looked like ‘run over by the disease’, therefore negative in laboratory tests. On the basis of symptoms and no other option, it was decided to give JD vaccine a try with the consent of owner.
A young male calf of Hariana breed (14 months old) was reared by CDHIFI, the NGO in Vrindavan. Mother of calf died due to dystocia during birth of this calf and was reared on external source of milk, Among livestock the NGO had only this calf. Though the calf was on high plane of nutrition (ad lib quality concentrate ration and fodder and was stall-fed) and in good management and hygienic conditions, however, calf was suffering from clinical JD (dark in colour unlike white colour of Hariana breed, physically weak and stunted without diarrhoea). On screening against MAP infection, the calf was negative in fecal microscopy, blood PCR and indigenous ELISA. The calf was regularly given Ivomec as first line of treatment against ecto and endo parasites. The experienced veterinarians of NGO tried all possible therapies for stunted growth, before referring to Animal Health Division of Central Institute for Research on Goats (CIRG), Makhdoom, Dist., Mathura. With the consent of NGO, the calf was vaccinated against JD.
‘Indigenous vaccine’ was developed at CIRG, Makhdoom using native ‘S 5’ strain, a new biotype (‘Indian Bison type’) of MAP (Sohal et al., 2009; Singh et al., 2013c) for the therapeutic management of JD in goats and sheep (Singh et al., 2010a; Singh et al., 2013b; Shroff et al., 2013). The cow and calf were vaccinated with 2 ml of ‘Indigenous Vaccine’ subcutaneously in middle of neck and were monitored at weekly interval, initially and later at monthly intervals. Monitoring parameters included physical condition, health (status of diarrhoea and weakness), production (growth rate, milk yield), sero–conversion and status of shedding of MAP in feces.
For diagnosis and monitoring following tests were used. In microscopy, nearly 2 gram of fecal sample was finely grounded in sterilized distilled water and centrifuged (4000 rpm for 45 min) at room temperature. Smear was prepared from middle layer, stained by Ziehl Neelsen (ZN) method and examined under oil immersion (100X) for acid–fast bacilli (AFB) indistinguishable to MAP. In IS900 blood–PCR, DNA isolated from blood samples was subjected to specific IS900 PCR (Singh et al., 2010b). Presence and yield of specific PCR product (413 bp) was analyzed by 2% agarose ethidium bromide gel electrophoresis. Indirect ELISA was used as per the protocol of Singh et al. (2007b) to know the status of MAP infection (S/P ratio method of Collins, 2002) and monitoring of immune response. S/P ratio of 1.0 to 10.0, 0.4 to 0.99, 0.25 to 0.39 and <0.25, were considered strong positive, positive, low positive and negative, respectively. Animal in positive and strong positive category were considered positive for MAP infection or as sero–converted after vaccination.
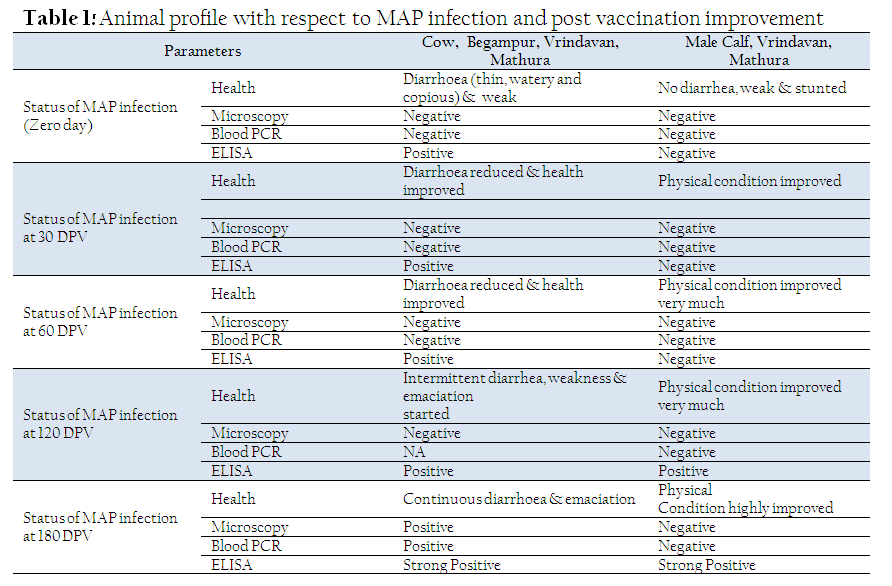
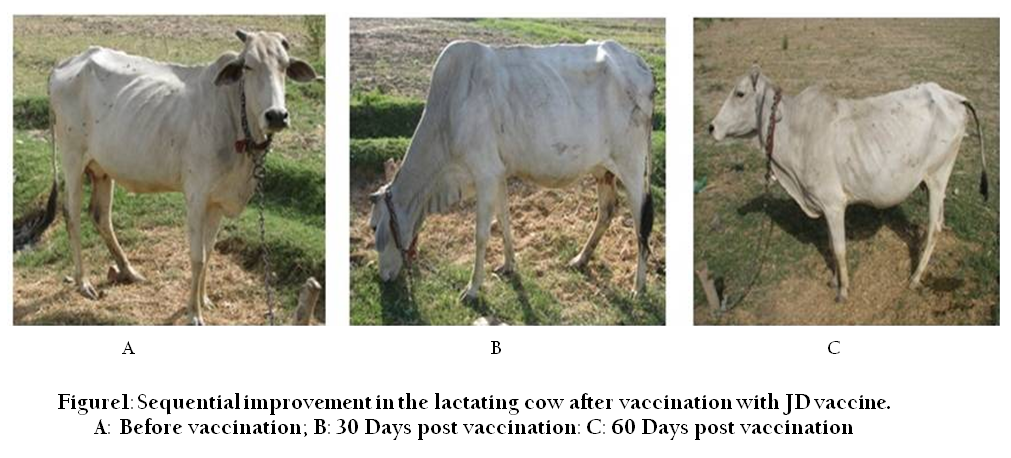
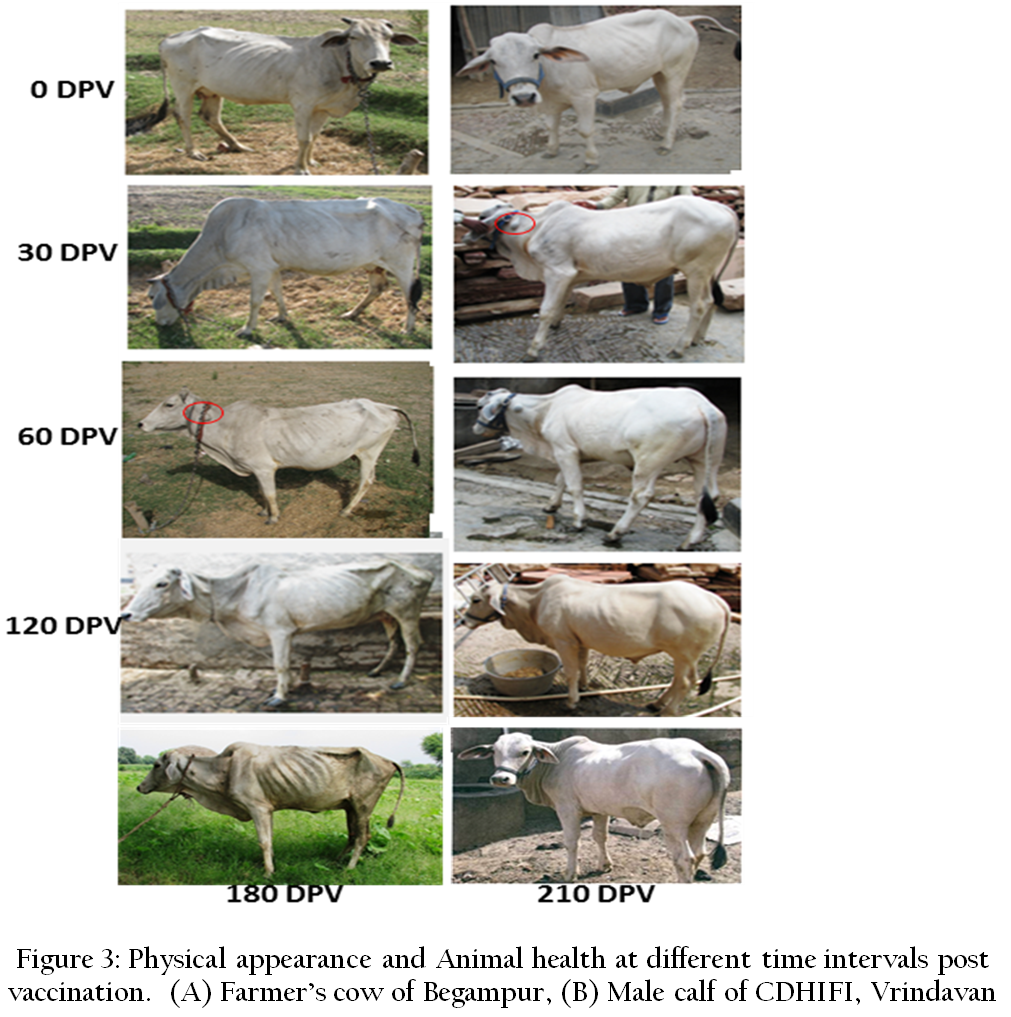
The cow was negative in fecal microscopy and blood PCR but was positive in ELISA before vaccination (Table 1). Cow started showing recovery two weeks after vaccination and physical condition improved considerably in two months post vaccination (Figure 1). Volume of the diarrhoea decreased whereas consistency of diarrhoea increased by 15–20%. Due to floods there was break in monitoring as village was surrounded by water and grazing area was inundated, therefore cow suffered further stress, After 4th month, when we went to see the cow, it has relapsed exhibiting watery diarrhoea and further deterioration in physical condition exhibiting emaciation and hide bound condition (Figure 3A). The size of ‘take’ was also reduced significantly. In this stage also cow was giving 500 ml of milk twice daily. The deterioration was mainly due to submerging of meager grazing area and it took more than one month for water to recede and still area was marshy and unfit for grazing.
In advanced stages of disease (clinical and advance clinical) vaccination was not successful (Singh et al., 2010a). In cases optimum nutrition as was case in goats at CIRG, the majority of goats (80–85%) recovered, however 15–20% goats with advance clinical JD were lost and could not recover (Singh et al., 2011).
In the present study also, either initial dose of vaccine was not optimum or cows needed booster dose after initial vaccination or immune system was damaged beyond repair. Since immune system in advance cases of JD is weak and under stress, therefore it needs due consideration before recommending increasing ‘initial loading dose’ or ‘booster dose’ as an option. However, in the cow booster vaccination after 2 months did not help, since already stress immune system was further damaged by initial dose. Reduced initial dose might have been a better option. In cow booster vaccine might have further stressed or damaged already fragile immune system leading to hastening the disease process and emaciation. Lactation, milking and depletion of feeding resources were other important stress factors that contributed to the failure of immune response, after the cow showed recovery from diarrhoea and improved in physical condition for two months. Though the cow was ‘over–run’ by disease, yet immune–system was working in initial 2 months after vaccination. Since cow was in positive category for the status of JD by ELISA. Native cow showed greater resilience to sustain the infection despite being in diarrhoea for last three years.
The male calf was negative in all three tests; fecal microscopy, blood PCR and indigenous ELISA (Table 1). This may be due to early stage of infection, one time sampling and dormancy (Singh et al., 2013d). Two weeks after vaccination calf developed very good take and started improving in body condition (Figure 2). Appetite increased and in next 4 months calf showed extremely good recovery and growth rate (Figure 3B).
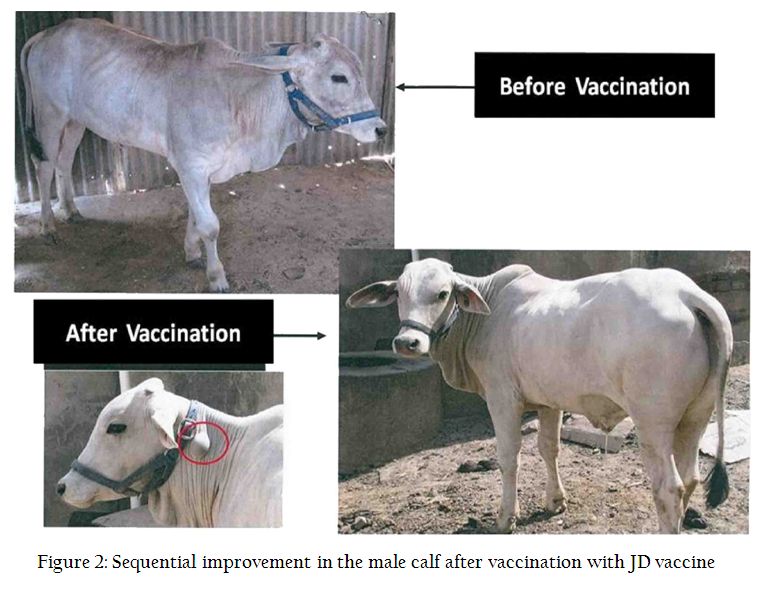
The calf bloomed in health and became shining white in colour. Monitoring sero–status of calf showed that it sero–converted and peak titers were achieved at 180 days post vaccination). It may be due to stress and partial damage to the immune system (mesenteric lymph nodes) due to MAP infection. Singh et al. (2010a and 2011) has shown that after vaccination all clinically affected goats, sero–converted and achieved peak titers by 75 to 150 days post vaccination using ‘indigenous JD vaccine’. Whereas in prophylactic vaccination of young kids sero–converted and achieved peak titers by 35 days post vaccination (Singh et al., 2007a). In subsequent monitoring calf showed consistent improvement except during July and August when calf could not get proper green fodder due to floods. Even after 7 months of vaccination, calf continued to maintain good ‘take’ (almost of same size as in the beginning) and good health. Despite calf was negative in laboratory tests but responded to ‘therapeutic management’ of JD using ‘indigenous goat based vaccine’.
The two case reports also exposed the limitation of diagnostic tests in JD and why all the infected animals cannot be detected in one time screening using single test. Therefore, diagnosis on the basis of one or two tests can be misleading and it is always handy to use multiple tests taking physical (weakness, stunting, diarrhoea) and production (low birth weight, low growth rate, lowered productivity) conditions into consideration, is always prudent and sometimes better indicator if used judiciously with discretion. In sub–clinical or initial stages of clinical JD calf though started to show symptoms but was not shedding MAP. Animals on optimum and good plane of nutrition may not hasten shedding of MAP in feces or in blood circulation or develop in-sufficient antibody titers. Therefore, it is advisable not to ignore physical symptoms as they are characteristic along with history. Treatment history and follow–up of routine health care schedule are important in diagnosis of JD in individual animals. Weakness in calf without diarrhoea was rare in cattle which is a usual symptom in goats and sheep. Since calf was routinely de–wormed, therefore had no predisposing factor for developing diarrhoea. Dose of 2 ml of goat based vaccine with optimum nutrition, seemed to work up to 7 months of vaccination (period for which calf was monitored) (Figure 3).
Study revealed endemicity of MAP infection in Indian native cattle as reported by Sharma et al. (2008). Study showed that animals suffering with clinical and advance clinical JD can be retrieved back to health and productivity using indigenous vaccine. Inactivated vaccine reduces incidence of clinical JD (Reddacliff et al., 2006; Singh et al., 2007a; Singh et al., 2013b), is cost effective and has therapeutic potential (Singh et al., 2010a; Bastida and Juste, 2011). Comparative efficacy of ‘indigenous vaccine’ developed at CIRG, Makhdoom was better over a commercial vaccine for some of parameters analyzed in an experimentally challenged trial in goats (Singh et al., 2007a). Therefore, indigenous goat based vaccine can be used for therapeutic management of JD in cattle and underlined role of stress factors (principally nutrition) in response to vaccination. Impact of candidate strain of vaccine was also observed by Uzonna et al. (2003) who reported that native field strain based paratuberculosis vaccine was more effective and efficacious than commercial vaccine. On same logic in this study also the goat based indigenous vaccine was used to treat clinical JD.
Study also underlined need for immediate attention for management and control of JD in the population of native domestic cattle. Response to specific treatment (vaccine) in the cow and calf confirmed the initial diagnosis based on clinical symptoms, where specific diagnostic tests failed.
CONFLICT OF INTEREST
No conflict of interest to declare.
ACKNOWLEDGEMENTS
Authors are thankful to CSIR, New Delhi for providing the funds and Director, CIRG, Makhdoom for providing the facilities.
REFERENCES
Bastida F and Juste RA (2011). paratuberculosis control: a review with a focus on vaccination. J. Immune. Based. Ther. Vaccines. 9: 8.
http://dx.doi.org/10.1186/1476-8518-9-8
PMid:22035107 PMCid:PMC3222599
Collins MT (2002). Interpretation of a commercial bovine paratuberculosis enzyme–linked immunosorbent assay by using likelihood ratios. Clin. Diag. Lab. Immunol. 9(6):1367–1371.
PMid:12414776 PMCid:PMC130105
FAO (2012). FAOSTAT, Food and Agriculture Organization, Rome.
Greenstein RJ and Collin MT (2004). Emerging pathogens: Is Mycobacterium avium subspecies paratuberculosis zoonotic. Lancet. 364(9432): 396–397.
http://dx.doi.org/10.1016/S0140-6736(04)16781-0
Harris NB and Barletta RA (2001). Mycobacterium avium subsp. paratuberculosis in veterinary medicine. Clin. Microbiol. Rev. 14(3): 489–512.
http://dx.doi.org/10.1128/CMR.14.3.489-512.2001
PMid:11432810 PMCid:PMC88986
Mishra P, Singh SV, Bhatiya AK, Singh PK, Singh AV and Sohal JS (2009). Prevalence of Bovine Johne's Disease (BJD) and Mycobacterium avium subspecies paratuberculosis genotypes in dairy cattle herds of Mathura district. Indian J. Comp. Microbiol. Immunol. Infect. Dis. 30(1): 23–25.
Reddacliff L, Eppleston J, Windsor P, Whittington R and Jones S (2006). Efficacy of killed vaccine for the control of paratuberculosis in Australian Sheep flocks. Vet. Microbiol. 115 (1–3): 77–90.
http://dx.doi.org/10.1016/j.vetmic.2005.12.021
PMid:16459030
Sharma G, Singh SV, Sevilla I, Singh AV, Whittington RJ, Juste RA, Kumar S, Gupta VK, Singh PK, Sohal JS and Vihan VS (2008). Evaluation of indigenous milk ELISA with m–culture and m–PCR for the diagnosis of bovine Johne's disease (BJD) in lactating Indian dairy cattle. Res. Vet. Sci. 84(1): 30–37.
http://dx.doi.org/10.1016/j.rvsc.2007.03.014
PMid:17544046
Shroff S, Chandel BS, Dadawala AI, Singh SV, Bhagat AG, Chauhan HC, Gupta S, Chaubey KK (2013). Evaluation of Indigenous vaccine in Patanwadi sheep naturally infected with clinical Johne's disease. Research Opinions in Animal & Veterinary Sciences. 3(9): 322–329.
Singh PK, Singh SV, Kumar H, Sohal JS and Singh AV (2010b). Diagnostic application of IS900 PCR using blood as a source sample for the detection of Mycobacterium avium subspecies paratuberculosis in early and subclinical cases of caprine paratuberculosis. Vet. Med. Int. 748621, doi: 10.4061/2010/748621, 1–8.
http://dx.doi.org/10.4061/2010/748621
Singh SV, Kumar N, Singh SN, Bhattacharya T, Sohal JS, Singh PK, Singh AV, Singh B, Chaubey KK, Gupta S, Sharma N, Kumar S, Raghava GPS (2013c). Genome Sequence of the 'Indian Bison Type' Biotype of Mycobacterium avium subsp. paratuberculosis Strain S5. Genome Announ. 1(1): e00005–13.
http://dx.doi.org/10.1128/genomeA.00005-13
PMid:23469332 PMCid:PMC3587920
Singh SV, Singh AV, Kumar A, Singh PK, Deb R, Verma AK, Kumar A, Tiwari R, Chakraborty S and Dhama K (2013d). Survival mechanisms of Mycobacterium avium subspecies paratuberculosis within host species and in the environment–A review. Natural Science. 5(6): 710–723.
http://dx.doi.org/10.4236/ns.2013.56088
Singh SV, Singh AV, Singh PK, Gupta S, Singh H, Singh B, VinodhKumar OR, Rajendiran AS, Swain N, Sohal JS (2013b). Evaluation of 'Indigenous vaccine' developed using 'Indian Bison Type' genotype of Mycobacterium avium subspecies paratuberculosis strain 'S5' of goat origin in a sheep flock endemic for Johne's disease: A three years trial in India. World Journal of Vaccines. 3(2): 52–59.
http://dx.doi.org/10.4236/wjv.2013.32009
Singh SV, Singh AV, Singh PK, Sohal JS and Singh NP (2007b). Evaluation of an indigenous ELISA for diagnosis of Johne's disease and its comparison with commercial kits. Indian. J. Microbiol. 47(3): 251–258.
http://dx.doi.org/10.1007/s12088-007-0046-2
PMid:23100673 PMCid:PMC3450340
Singh SV, Singh PK, Singh AV, Gupta S, Chaubey KK, Singh B, Kumar A, Srivastav A and Sohal JS (2013a). Bio–burden and bio–type profiles of Mycobacterium avium subspecies paratuberculosis infection in suspected population of domestic livestock in India. Int. J. Current Res. 5(7): 1897–1901.
Singh SV, Singh PK, Singh AV, Sohal JS and Sharma MC (2010a). Therapeutic effects of a new 'Indigenous Vaccine' developed using novel native 'Indian Bison type' genotype of Mycobacterium avium subspecies paratuberculosis for the control of clinical Johne's disease in naturally infected goatherds in India. Vet. Med. Int. doi:10.4061/2010/351846.
http://dx.doi.org/10.4061/2010/351846
Singh SV, Singh PK, Singh AV, Sohal JS, Gupta VK and Vihan VS (2007a). Comparative efficacy of an indigenous 'inactivated vaccine' using highly pathogenic field strain of Mycobacterium avium subspecies paratuberculosis 'Bison type' with a commercial vaccine for the control of Capri–paratuberculosis in India. Vaccine. 25: 7102–7110.
http://dx.doi.org/10.1016/j.vaccine.2007.07.054
PMid:17804124
Singh SV, Singh PK, Singh MK, Singh AV and Sohal JS (2011). Therapeutic potential of Johne's disease vaccine: A follow up post vaccination study in a goatherd of endangered Jamunapari breed, naturally infected with Mycobacterium avium subspecies paratuberculosis. International Journal of Livestock Production. 2(13): 192–204.
Sohal JS, Sheoran N, Narayanasamy K, Brahmachari V, Singh SV and Subodh S (2009). Genomic analysis of local isolate of Mycobacterium avium subspecies paratuberculosis. Vet. Microbiol. 134(3–4): 375–82.
http://dx.doi.org/10.1016/j.vetmic.2008.08.027
PMid:18838235
Uzonna JE, Chilton P, Whitlock RH, Habecker PL, Scott P, and Sweeney RW (2003). Efficacy of commercial and field–strain Mycobacterium paratuberculosis vaccinations with recombinant IL–12 in a bovine experimental infection model. Vaccine. 21(23): 3101–3109.
http://dx.doi.org/10.1016/S0264-410X(03)00261-5



