Journal of Infection and Molecular Biology
Research Article
Journal of Infection and Molecular Biology 2 (3): 35 – 38Prevalence of Hepatitis B and C Infection in Pakistan
Abdul Basit*, Kashif Rahim, Iqbal Ahmad, Mehwish Shafiq, Sameerah Mushtaq, Humera Shaheen, Ilyas Khan
-
Department of Microbiology, Kohat University of Science and Technology (KUST), Khyber PakhtunKhwa, 26000, Pakistan
*Corresponding author:aabdul.9090@gmail.com
ARTICLE CITATION:
Basit A, Rahim K, Ahmad I, Shafiqe M, Mushtaq S, Khan I, Shaheen H (2014). Prevalence of hepatitis B and C infection in Pakistan. J. Inf. Mol. Biol. 2 (3): 35 – 38.
Received: 2014–04–20, Revised: 2014–05–18, Accepted: 2014–05–19
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/jimb.2307-5465/2.3.35.38
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Hepatitis is an important global health problem especially in developing countries. Patients with HBV and HCV are at great threat for increasing chronic liver diseases. The present study was carried out to estimate the prevalence of HBV and HCV in hospital patients of Pakistan Institute of Medical Sciences, Islamabad (PIMS). A total of 845 patients were screened for hepatitis over the period of three months (1st June to 31st August 2011). All patients underwent screening for HB–Ag and anti–HCV antibodies by ELISA. The overall prevalence of HBV and HCV was found to be (2.8%) and (18.9%) respectively. Moreover Co–infection (both HBV and HCV) was found to be (0.7%). High prevalence was found in males (24%) followed by females (20.3%) with statistically significant association (P = 0.0217) [OR=0.85 (CI = 0.6–1.17)]. Similarly, HBV and HCV were found to be more common among married individuals (23.1%) compared to un–married (20.7%) (P = 0.1675) [OR = 0.89 (CI = 0.62– 1.27)]. Significance association was found among the age groups (P = 0.0231). The higher prevalence of HBV and HCV was recorded in patients with age group of greater than 60 years (57.2%) [OR = 0.39 (CI= 0.29 – 0.53)] followed by age group of 40–60 years (18.3%) [OR = 1.2 (CI = 0.9– 1.6)]. In conclusion, the present study provides the preliminary information about HBV and HCV prevalence due to lack of public health awareness on transmission of disease. More sensitive methods for detection of hepatitis virus, management and control to overcome its future spread are required. It is recommended that public health authorities should educate the general public regarding prevention.
INTRODUCTION
Hepatitis B and Hepatitis C infection is a major health problem worldwide, especially in Asia, Africa and other developing countries (Ujjan et al., 2012). These are the hepato–tropic viruses leading to significant morbidity and mortality throughout the world (Hafeez–ud–din et al., 2012). Hepatitis is characterized by the inflammation of liver and both hepatitis B and C can lead to liver failure, cirrhosis of liver and may ultimately lead to end stage liver disease. Hepatitis C infection has serious sequale; it can lead to acute hepatitis, chronic hepatitis or a chronic carrier state and hepato–cellular carcinoma (HCC). More than half of all HCV infections lead to chronic liver disease, and majority of HCC cases in Pakistan are associated with Hepatitis C virus (HCV) (Umar and Bilal, 2012). No vaccine is available for HCV as yet and treatment cost is very high
Hepatitis mainly transmitted as a result of blood transfusion, injury with contaminated instruments, sharing of used needles, by sexual contact and also through parental transmission from mother to child. The major modes of HCV transmission in Pakistan are use of contaminated needles and instruments in medical practice, unsafe blood and blood product transfusion, intravenous drug use, face and armpit shaving with unsterilized instruments by barbers and poor personal hygiene habits (Jamil et al., 2010).
Different methods used for the diagnosis of hepatitis including immunochromatography (ICT), Enzyme Linked Immunosorbent Assay (ELISA) and Polymerase Chain Reaction (PCR) (Hayder et al., 2012). ELISA is most important and referred screening technique and having an accuracy of about 99.9% (Torane and Shastri, 2008). Moreover both ELISA and PCR methods are expensive and are use in well equipped labs and major tertiary care hospitals. Comparatively, rapid test for diagnosis mostly ICT kits are used because of quicker, easy to perform and are less expensive (Hayder et al., 2012).
Based on global estimation of 2006, as many as 175 million persons are infected with HCV alone where as HBV is responsible for 500,000 to 1,000,000 deaths annually worldwide (Aziz et al., 2010). High prevalence rates have been found in South East Asian countries such as Thailand, India, and Malaysia (Khan, 2010). In Pakistan the prevalence of HBV is reported as 10% and prevalence of HCV is 6.7% in women and 1.3% in children in 2010 (Khan, 2010). Multiple studies have been conducted regarding prevalence rate of Hepatitis B infection based on various population groups in Pakistan. According to various study groups, the prevalence rate of Hepatitis B has been reported as 2–10% among healthy blood donors, 5–9% among health care personnel, 3.6 to 18.66% among the general population, 3–16% among pregnant women (Khan, 2010; Aziz et al., 2010). A recent study found Hepatitis C prevalence within provinces as 5% in Sindh, 6.7% in Punjab, 1.1% in Khyber PakhtunKhwa and 1.5% in Baluchistan. For Hepatitis B Figure was 2.55% in Sindh, 2.4% in Punjab, 1.31% in PakhtunKhwa and 4.3% in Baluchistan (Siddique and Sohag, 2010).
The aim of current study was to estimate the prevalence of Hepatitis B and C in visiting patients to hospital at Pakistan Institute of Medical Sciences (PIMS), Islamabad.
MATERIALS AND METHODS
A study was carried out in Pakistan Institute of Medical Sciences (PIMS), Islamabad from, 1st June to 31st August 2011. A total 845 blood samples were collected from clinically suspected patients for Hepatitis B and C. Individual information on history, sex, age and maternal status were obtained by interviewing the patients. The patients were screened for Hepatitis B surface Ag (HBs–Ag) and Anti–HCV antibody by ELISA Kits (The Bio–kit ELISA system, BEST 2000), according to the instruction of the manufacturer.
Data were analyzed using SPSS 16.0 statistical software. Chi–square was utilized in assessing statistical significance of association. Simple logistic regression analysis was performed to measure association of outcome with each independent variable; odds ratios (OR) and 95% confidence intervals (CI) were calculated for each risk factor.
RRESULT
Prevalence of Hepatitis B and C in present study were classified according to questioners were assembled in sex, marital status and age wise.
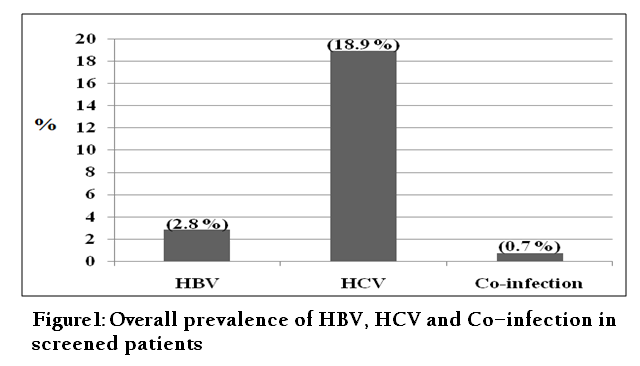
Out of 875 patients, a total 190 (22.4%) patients were found positive for HBV and HCV. Among these 24 (2.8%) and 160 (18.9%) were positive for HBV and HCV respectively and 06 (0.7%) patients have co–infection of HBV and HCV (Figure 1).
Out of 875 patients, 482 were male and 363 were female. Among males patients HBV, HCV and co–infection were present in 15 (3.1%), 97 (20.1%) and 04 (0.8%) respectively with overall prevalence of 24% (Table 1). Similarly among females patients HBV, HCV and co–infection were present in 09 (2.4%), 63 (17.3%) and 02 (0.5%) respectively with overall prevalence of 20% (Table 1). A statistically significant association was found between male and female patients (P = 0.0217) [OR=0.85 (CI = 0.6–1.17)] (Table 4).


Out of 875 patients 604 married and 241 were unmarried. Among the married patients HBV HCV and co infection was found 17 (2.8%), 119 (19.7%) and 04 (0.6%) respectively with overall prevalence of 23.1% (Table 2). Similarly, among the unmarried patients HBV HCV and co infection was found 07 (2.9%), 41 (17%) and 02 (0.8%) respectively with overall prevalence of 20.7% (Table 2). A statistically significant difference was found between married and un–married patients (P = 0.1675) [OR = 0.89 (CI = 0.62– 1.27)] (Table 4).
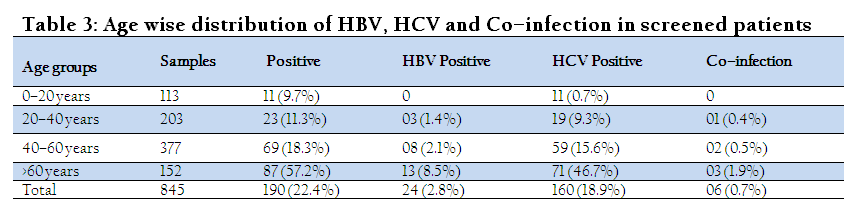
The HBV frequency regarding the age group of patients ranging from 20–40, 40–60 and greater than 60 years of age was found 03 (1.4%), 08 (2.1%) and 13 (8.5%) respectively (Table 3). Similarly, HCV in patients with age group ranging from 0–20 years, 20–40, 40–60 and greater than 60 years of age was found 11 (9.7%), 19 (9.3%), 59 (15.6%) and 71 (46.7%) respectively. Moreover, Co–infection was found in patients with age group of 20–40, 40–60 and greater than 60 years of age was found 01 (0.4%), 02 (0.5%) and 03 (1.9%) respectively (Table 3). Statistically significant association was found among the age groups of these patients (P = 0.0231) (Table 4).

DISCUSSION
Hepatitis is a major health problem worldwide. Numerous studies have been conducted regarding prevalence of Hepatitis B and C infection in various population groups in Pakistan.
In present study anti–HCV positivity was found much higher compared to Hbs–Ag. Gul–e–atif et al., (2009) in their study reported the prevalence of Hepatitis B and C in patients was (2.65%) and (10.42%), respectively. Their findings are much similar to findings of the present study, reported high prevalence of Hepatitis C compared to Hepatitis B. In another study of Irfan et al., (2004) also reported the high prevalence of Hepatitis C compared to Hepatitis B. Moreover, the Hepatitis B prevalence in present study was found 2.8%. Chaudhary et al., (2007) and Gul–e–atif et al., (2009) in their studies also reported the prevalence of Hepatitis B was 2.8% and 2.7% respectively. So these findings are in consistent with the findings reported by other studies, as the prevalence of Hepatitis B is between 2.11% to 5.46% in different parts of country (Chaudhary et al., 2007). In present study Co–infection (of Hepatitis B and C) was observed in 0.7% patients. Similar findings was also observed by Gul–e–atif et al., (2009), reported the mixed infection in patients was found to be 0.16%. Risk factor among the positive cases might be the surgical intervention, because it has been estimated that people of these areas more prefers the intramuscular injections for fever and general ailment. These injections are more often provided by informal, untrained health workers. Moreover, patients more eager to pay an extra physician’s fee for injections but will not pay for oral medications. Furthermore, sterility of injections not maintained frequently, due to financial limitations and lack of awareness among the healthcare providers and the population in general (Ali et al., 2009)
Males had higher rates of HBs–Ag and anti–HCV antibodies compares to females (Wasfi and Sadek, 2011). In present study similar findings were obtained regarding high prevalence of Hepatitis B and C in males compared to females. In another study, Nafeh et al., (2000) reported high the prevalence of anti–HCV among males compared to females in Egypt. Results of the present study were also in agreement with the findings of Chaudhary et al., (2007), reported high prevalence of anti–HCV antibodies and HBs–Ag among males. High prevalence of Hepatitis in males might be due to fact that males make more common visits to barber and they may be more probably to get wounded and may share equipments. Moreover, men also are more likely to have many sex partners and follow unprotected sex.
In the present study the Hepatitis B and C prevalence in married patients was found higher followed by un–married patients. The result of the present study was in agreement with the results of Ayele and Solomon, (2013), reported the prevalence of Hepatitis B and C higher in married patients. Similarly Adekeye et al., (2013) in their study also reported the higher prevalence of Hepatitis B and C in married patients compared to un–married. It might be due to lack of awareness or education in people that has pre–exposure prior to marriage which is then transmitted to her or his spouse.
Individuals aged greater than 60 years had the highest prevalence of Hepatitis B and C followed by the age group of 40–60 years. Finding of the present study were also reported in many studies that the prevalence of hepatitis is increases until the age of 30 years, and it rises even higher among those over the age of 40 years (Rey–Cuille et al., 2012; Abdel–Hady and Kelly, 2013; Triki et al., 1997).
It was concluded from the present study that prevalence of Hepatitis B is relatively low compared to Hepatitis C. Moreover, high prevalence was recorded among males than females. It is recommended that great care should be implemented during surgical procedures or treatments and blood transfusions. Furthermore awareness campaign against Hepatitis B and C infections should be conceded to educate the general population on the risk factors and mode of spread in order to reduce the rate of infection.
REFERENCES
Abdel–Hady M, Kelly D (2013). Chronic hepatitis B in children and adolescents: epidemiology and management. Pediatric Drugs. 15(4): 311 – 317.
http://dx.doi.org/10.1007/s40272-013-0010-z
PMid:23529864
Adekeye AM, Chukwuedo AA, Zhakom PN, Yakubu RS (2013). Prevalence of Hepatitis B and C among Blood Donors in Jos South LGA, Plateau State, Nigeria. Asian J. Med. Sci. 5 (5): 101 – 104.
Ali SA, Rafe MJ, Donahue, Qureshi H, Vermund SH (2009). Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors. Int. J. Infect. Dis. 13(1): 9 – 19.
http://dx.doi.org/10.1016/j.ijid.2008.06.019
PMid:18835208 PMCid:PMC2651958
Ayele AG, Solomon GS (2013). Prevalence and Risk Factors of Hepatitis B and Hepatitis C Virus Infections among Patients with Chronic Liver Diseases in Public Hospitals in Addis Ababa, Ethiopia. Trop. Med. 2: 1 – 7.
Aziz S, Khanani R, Noorulain W (2010). Hepatitis B and C in rural and periurban Sindh. J. Pak. Med. Assoc. 60: 853 – 857.
PMid:21381619
Chaudhary IA, Samiullah, Khan SS, Masood R, Sardar MA, Mallhi AA (2007). Seroprevalence of hepatitis B and C among the healthy blood donors at Fauji Foundation Hospital, Rawalpindi. Pak. J. Med. Sci. 23: 64 –67.
Gul–e Atif, Jamal N, Abbas H (2009). Seropositivity of Hbs Ag and Anti HCV in Rawalpindi and Islamabad and analysis of risk factors. Ann. Inst. Med. Sci. 5: 242 – 244.
Hafeez–ud–din, Siddiqui TS, Lahrasab W, Sharif MA (2012). Prevalence of Hepatitis B and C in healthy adult males of paramilitary personnel in Punjab. J. Ayub Med. Coll. Abbottabad. 24: 3 – 4.
Hayder I, Ahmed W, Alam SE (2012). Comparison of different ICT Kits for HBs–Ag andAnti–HCV using gold standard ELISA. Pak. J. Med. Res. 51: 72 – 76.
Irfan AM, Sajjad HM, Sabahat I, Rashad S, Waheed UZT, Asif M (2004). Seroprevalence of Hepatitis B and C in young adults seeking recruitment in armed forces. Pak. Arm. Forc. Med. J. 2: 5 – 8.
Jamil MS, Ali H, Shaheen R, Basit A (2010). Prevalence, knowledge and awareness of Hepatitis C among residents of three union councils in Mansehra. J. Ayub Med. Coll. Abbottabad. 22: 10– 14.
Khan N (2010). Effect of gender and age on the knowledge, attitude and practice regarding hepatitis B and C and vaccination status of hepatitis B among medical students of Karachi, Pakistan. J. Pak. Med. Asso. 60: 450 – 455.
PMid:20527642
Nafeh MA, Medhat A, Shehata M, Mikhail NN, Swifee Y, Abdel–Hamid M, Watts S, Fix AD, Strickland GT, Anwar W, Sallam (2000). Hepatitis C in a community in upper Egypt: cross–sectional survey. Amer. J. Trop. Med. Hyg. 63:236 – 241.
PMid:11421370
Rey–Cuille MA, Seck A, Njouom R, Chartier L, Sow HD, Njankouo M, Rousset D, Giles–Vernick T (2012). Low immune response to hepatitis B vaccine among children in Dakar, Senegal. PLoS One. 7(5): 15 – 18.
http://dx.doi.org/10.1371/journal.pone.0038153
PMid:22666468 PMCid:PMC3364238
Siddique KM, Sohag AA (2010). Hepatitis B and C; Share of young rural populace of Sindh. Med. Chan. 16: 215 – 218.
Torane VP, Shastri JS (2008). Comparison of ELISA and rapid screening tests for the diagnosis of HIV, hepatitis B and hepatitis C among healthy blood donors in a tertiary care hospital in Mumbai. Indian J. Med. Microbiol. 26: 284 – 285.
http://dx.doi.org/10.4103/0255-0857.42071
PMid:18695340
Triki H, Said N, Ben Salah A, Arrouji A, Ben Ahmed F, Bouguerra A, Hmida S, Dhahri R, Dellagi K (1997). Seroepidemiology of hepatitis B, C and delta viruses in Tunisia. Trans. R. Soc. Trop. Med. Hyg. 91: 11 – 14.
http://dx.doi.org/10.1016/S0035-9203(97)90374-6
Ujjan I, Aurangzeb M, Memon RA, Memon ZY (2012). Prevalence of Hepatitis B Virus (HBV) in association of Hepatitis Delta Virus (HDV). Med. Chennal. 4: 53 – 57.
Umar M, Bilal M (2012). Hepatitis C, A Mega Menace: A Pakistani Perspective. J. Pion. Med. Sci. 2: 68 – 72.
Wasfi OAS, Sadek NA (2011). Prevalence of hepatitis B surface antigen and hepatitis C virus antibodies among blood donors in Alexandria, Egypt. Health J. 3: 238 – 242. East. Medit.



