Advances in Pharmaceutical and Ethnomedicines
Research Article
Advances in Pharmaceutical and Ethnomedicines. 2 (1): 14 – 17Comparative Evaluation of Side Effects of Typical and Atypical Antipsychotics in Psychotic Patients at Punjab Institute of Mental Health, Lahore, Pakistan
Allah Bukhsh1*, Zulfiqar Ali2, Muhammad Tayyab2, Zubda Gohar1, Sameen Amjad1, Syeda Sabika Raza Abidi1, Nadia Safdar1
- Institute of Pharmaceutical Sciences, University of Veterinary and Animal Sciences, Lahore, Pakistan
- Punjab Institute of Mental Health, Lahore, Pakistan
*Corresponding author:abukhsh@uvas.edu.pk
ARTICLE CITATION:
Bukhsh A, Ali Z, Tayyab M, Gohar Z, Amjad S, Abidi SSR, Safdar N (2014). Comparative evaluation of side effects of typical and atypical antipsychotics in psychotic patients at Punjab Institute of Mental Health, Lahore, Pakistan. Adv. Pharm. Ethnomed. 2 (1): 14 -17.
Received: 2014–03–16, Revised: 2014–04–01, Accepted: 2014–04–02
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.ape/2014/2.1.14.17
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The use of antipsychotics has been widely increased in the management of psychotic disorders. The significant side effect reported by the use of antipsychotics is extrapyramidal symptoms (EPS) such as pseudoparkinsonism, akathesia, dyskinesia and dystonia. Many studies have been conducted to evaluate the relationship between antipsychotics and EPS. In this single blind and cross sectional study, comparative evaluation of extrapyramidal symptoms (EPS) and other side effects was made between two antipsychotic classes in 60 patients with various psychotic problems at Punjab Institute of Mental Health, Lahore, Pakistan. Patients’ condition regarding side effects was evaluated. EPS occurrence rate was much higher in patients receiving typical antipsychotics (73%) as compared to those taking atypical type (27%). It was also observed that the patients having bipolar disorder (53%) have increase tendency to develop EPS than schizophrenic patients (47%). EPS decrease significantly when treatment was switched from typical to atypical antipsychotics. In addition to EPS other side effects caused by atypical antipsychotics included weight gain in 2 patients (10%) and amenorrhea in 3 out 11 female patients (27%). This study confirmed that the patients taking atypical antipsychotics were more stable with fewer incidences of EPS.
INTRODUCTION
The most efficient treatment for psychosis is the use of psychotropic medication also known as neuroleptic agents (Leitner I et al., 2003). Antipsychotics are classified as typical or conventional (chlorpromazine, raclopride, thioridazine, haloperidol) and atypical or newer antipsychotics (Perlapine, quitiapine, melperone, sertindole, olanzapine, loxapine, molindone, remoxipride, clozapine.). All of them block dopamine (D2) receptors but some of atypical antipsychotics have the ability to block serotonin (5HT–2A) receptors (Goldstein JM, 2001; Citrome L, 2012). 80% blockade of D2 receptors is required for antipsychotic effect (Rang HP et al., 2007). The difference lies on the basis of receptor binding and the occurrence of EPS (Rang HP et al., 2007).
D2 receptor blockade causes motor disturbances including acute dystonia and tardive dyskinesia and Parkinson like symptoms called as extra pyramidal symptoms (EPS) (Goldstein JM, 2001; Rang et al., 2007). Newer generation has better safety profile as they are loosely bind to D2 receptors than dopamine therefore they are less associated with EPS (Goldstein JM, 2001; Tandon R, 2002; Kapur S and Seeman P, 2001). To reduce the development of EPS, adjunctive therapy is required (Cowen P et al., 2012). For this purpose anticholinergic medication is administered concurrently which includes biperidone or procyclidine but these can worsen the tardive dyskinesia and produce psychotic exacerbation (Cowen P et al., 2012). Atypical antipsychotics are widely used as first line treatment to minimize side effects (Letmaier M et al., 2006; Raja M and Azzoni A, 1996). The major side effects caused by atypical antipsychotics are metabolic side effects (QTC interval prolongation, myocarditis, sexual side effects, weight gain, diabetes mellitus type II, and hyperlipidemia), cataract and low proportion of EPS (Ucok A and Gaebel W, 2008).
The patients having bipolar disorder have increase tendency to develop EPS than schizophrenic patients (Ertugrul A and Meltzer HY, 2013; Letmaier M et al., 2006). Women using typical neuroleptics have tendency to develop more EPS than those women using atypical as compared to men (more EPS with atypical antipsychotics (Ertugrul A and Meltzer HY, 2013). Elderly patients are more prone to cause EPS as compared to young ones (Rang et al., 2007). The occurrence of EPS is also affected by dose. EPS caused by haloperidol, risperidone and olanzapine are directly related with the increase in dose .While for clozapine and quetiapine the relationship among dose and EPS is not significant (Goldstein JM, 2001; Ucok A and Gaebel W, 2008). Atypical antipsychotics are mainly used through oral route but are unavailable in injectable form and quite expensive; therefore patients are still using traditional neuroleptics and suffering from EPS (Raja M and Azzoni A, 1996).
The study presented here sought to evaluate the safety and tolerability (treatment emergent EPS) of antipsychotics in ambulatory and hospitalized patients with psychotic disorders.
MATERIALS AND METHODS
A concurrent, cross–sectional and single blind study was conducted at Punjab Institute of Mental Health, Lahore, Pakistan, which is a public sector tertiary care hospital with specialized diagnostic and treatment facilities in psychotic problems. During a 10 weeks study, from September to November 2013, data was collected from 60 patients suffering with various psychotic problems. Patients (both ambulatory and hospitalized) age ranging from 5–70 years (both male and female patients) with the various psychotic diseases was recruited in this study. Children below 5 years, geriatrics above 70 years of age, and, pregnant and lactating females were excluded from the study. Data was collected from patient medication profile and patient interview with the help of physician on follow–ups by observing the signs and symptoms that appeared in the patients after taking the medication. The main side effects observed were EPS, body weight gain and Hyperprolactemia (amenorrhea) and results were analyzed by using the Statistical Package for Social Sciences (SPSS), version 16.0.
RESULTS AND DISCUSSION
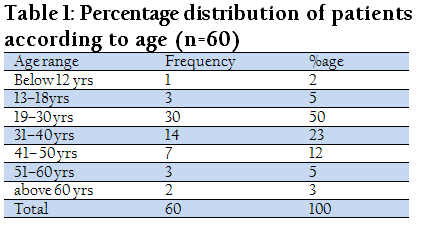
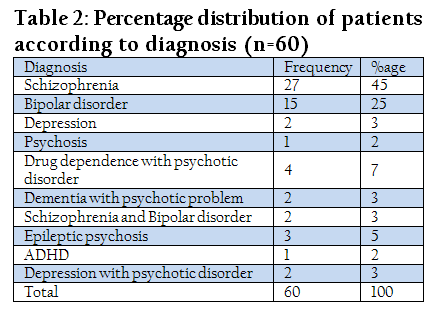
It was observed that majority of the patients with psychotic problems were male 40 (70%) and 20 (30%) were females, out of which 25 (42%) were institutional patients whereas 35 (58%) were ambulatory patients. The data collected showed that maximum patients were of age ranging from 19 to 30 years (50%) followed by 31–40 years (23%), 41–50 years (12%), 51–50 years (5%), 13–18 years (5%), above 60 years (3%), and below 12 years (2%) as shown in Table 1. The patients were mainly diagnosed with Schizophrenia (45%), Bipolar disorder (25%), Depression (3%), Psychosis (2%), Attention deficit hyperactivity disorder (ADHD) (2%), Epileptic psychosis (5%), Drug dependence with psychotic disorder (7%), Depression with psychotic disorder (3%), Dementia with psychotic disorder (3%) and Schizophrenia with Bipolar disorder (3%). Majority of the patients were suffering with Schizophrenia and least were seen with ADHD and psychosis as shown in Table 2.
All antipsychotics are dopamine (D2) receptor blocker (Tandon R, 2002). Typical antipsychotics are tightly bound to D2 receptors, so they stay for long time. The receptors are continuously bombarded with the drug so it creates not only an antipsychotic effect but also motor side effects (EPS). Tighter blockade results in increased risk of EPS (Tandon R, 2002). Whereas, atypical antipsychotics are loosely bound to the D2 receptors, with more rapid dissociation as compared to the conventional agents, leading to fewer motor side effects (Kapur S and Seeman P, 2001). No sufficient data was available to compare the incidence of EPS with the use of typical antipsychotics because atypical antipsychotics are used as a 1st line therapy while the use of typical anti psychotics is minimized due to its side effects and only used in emergency conditions as injectable form or where their use cannot be avoided (Raja M and Azzoni A, 1996). But the study was conducted in Pakistan that is a developing country where typical antipsychotics are still in use because they are economical. Minimum doses of the drugs were given to the patients as recommended by the World Psychiatric Association (McGorry P, 2005). In this study 40 (67%) patients were prescribed with atypical antipsychotics and 20 (33%) patients were prescribed with typical antipsychotics. Among atypical anti psychotics risperidone, olanzapine and quitiapine were given to 26 (43%), 12 (20%) and 2 (3%) patients respectively. 20 (33%) patients were prescribed with haloperidol (the only typical antipsychotic drug prescribed during the study) as shown in the Figure 1.
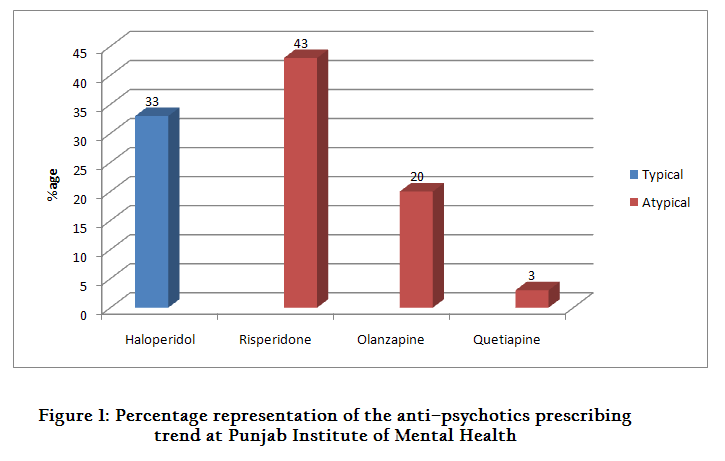
Figure 1: Percentage representation of the anti–psychotics prescribing trend at Punjab Institute of Mental Health
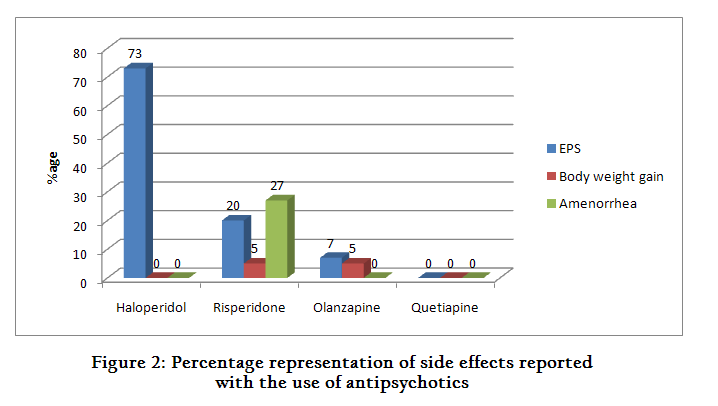
Out of total 60 patients, 20 (33%) patients were spotted with side effects. 15 (75%) patients were observed with EPS, 2 (10%) with body weight gain and 3 (27%) with amenorrhea as shown in Table 3. According to a study conducted in University of Michigan Medical Centre, Ann Arbor, Michigan in 2002, the hierarchy of occurrence of EPS was Risperidone > Olanzapine = Ziprasidone > Quetiapine > Clozapine (Tandon R, 2002). In our study, Out of the 15 patients observed with EPS, 11 (73%), 3 (20%) and 1 (7%) patients were taking haloperidol, risperidone and olanzapine respectively. Haloperidol was associated with more EPS and in case of atypical anti psychotic drugs, risperidone had increased tendency to cause EPS.

The data obtained from a study conducted in Pennsylvania in 1999 indicated that higher doses of risperidone increase the prolactin levels leading to amenorrhea (Petty RG, 1999). In our study 3 (27%) out of 11 females taking atypical antipsychotics were found to have amenorrhea with the use of risperidone (Figure 2) and none of the female patients taking haloperidol or olanzapine were seen with this side effect which is in compliance with a study conducted in Indiana (2000) (David SR, 2000).
Body weight gain is a common side effect associated with the use of atypical antipsychotics. The mechanism for this drug induced weight gain is not yet understood although serotonin (5HT2c) and Histamine (H1) receptor blockade may likely to contribute in this regard (Tandon R, 2002; Nasarallah H, 2003; Reynolds GP et al., 2006). The propensity of atypical antipsychotics to cause weight gain varies with long–term treatment. According to a study conducted in USA (2003), Clozapine and olanzapine were associated with largest body weight gain and smallest with quetiapine and ziprasidone whereas moderately body weight changes were associated with risperidone which were dose independent (Nasarallah H, 2003). Our study showed 2 (10%) patients with increased body weight, 1 (5%) with olanzapine and 1 (5%) with risperidone (Figure.2)
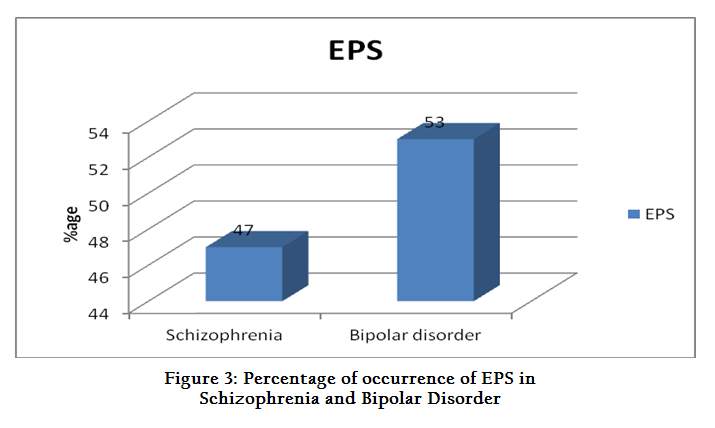
A study done in Turkey and USA (2003) (Ertugrul A and Meltzer HY, 2013) and Austria (2006) (Letmaier M et al., 2006) related that the patients having bipolar disorder develop EPS more frequently as compared to those patients having schizophrenia. This is one of the main reasons to prefer the use of atypical antipsychotics for the treatment of bipolar disorder. In our study, 7 (47%) and 8 (53%) patients diagnosed with schizophrenia and bipolar disorder respectively reported EPS (figure 3) which showed that the patients suffering from bipolar disorder were associated with more EPS as compared to the patients diagnosed with schizophrenia.
To reduce the adverse effects of typical antipsychotics that is, the development of EPS, adjunctive therapy is required. For this purpose anticholinergic medication is administered concurrently which includes biperidone or procyclidine (Ertugrul A and Meltzer HY, 2013). In our study, to manage the EPS reported by the use of antipsychotic drugs, procyclidine (5–30mg daily) was used but a routine use of anticholinergic drugs is not recommended in tardive dyskinesia because they increase its severity (Cowen P et al., 2012). Atypical antipsychotics are mainly used through oral route but unavailable in injectable form and are quite expensive; therefore patients are still using traditional neuroleptics and suffering from EPS (Ucok A and Gaebel W, 2008).
CONCLUSION
After the study we concluded that the prescribing trend in Punjab Institute of Mental Health, Lahore were somehow in accordance with the international prescribing trend which is appreciable. Limiting the use of typical antipsychotic drugs to emergency conditions only (as they are available in injectable form) will minimize the incidence of EPS, thus increasing the compliance of patients to antipsychotic therapy that would ultimately lead to better quality of life. Moreover, the role of pharmacist in designing the treatment strategies, counseling and patient education regarding the safe use of medicines should be encouraged in our society.REFERENCES
Citrome L (2012). Oral Antipsychotic Update: A Brief Review of New and Investigational Agents for the Treatment of Schizophrenia. CNS Spectrums. 17:1–9
http://dx.doi.org/10.1017/S1092852912000727
PMid:23448847
Cowen P, Harrison P and Burns T (2012). Shorter Oxford Textbook of Psychiatry, Oxford University Press, Italy 6th Edition
http://dx.doi.org/10.1093/med/9780199605613.001.0001
David SR, Taylor CC, Kinon BJ and Breier A (2000). The effects of olanzapine, risperidone, and haloperidol on plasma prolactin levels in patients with schizophrenia. 22(9): 1085–96
Ertugrul A and Meltzer HY (2013). Antipsychotic drugs in bipolar disorder. International Journal of Neuropsychopharmacology. 6: 277–284.
http://dx.doi.org/10.1017/S1461145703003560
PMid:12974994
Goldstein JM (2001). The new generation of antipsychotic drugs: how atypical are they? International Journal of Neuropsychopharmacology. 3(4): 339–349
http://dx.doi.org/10.1017/S1461145700002042
PMid:11343614
Kapur S and Seeman P (2001). Does fast dissociation from the dopamine 2 receptor explain the action of atypical antipsychotics? a new hypothesis. Am J Psychiatry. 158:360–369
http://dx.doi.org/10.1176/appi.ajp.158.3.360
Leitner I, Rieder NP, Willeit M and Kasper S (2003). Quetiapine in a delusional depressed elderly patient: no EPS and a favourable outcome. International Journal of Neuropsychopharmacology. 6: 199–200
http://dx.doi.org/10.1017/S1461145703003328
PMid:12890313
Letmaier M, Schreinzer D, Reinfried L, Glauninger G, Thierry N, Kapitany T and Kasper S (2006). Typical neuroleptics vs. atypical antipsychotics in the treatment of acute mania in a natural setting. International Journal of Neuropsychopharmacology. 9: 529–537
http://dx.doi.org/10.1017/S1461145705006073
PMid:16191207
McGorry P (2005). International clinical practice guidelines for early psychosis. British Journal of Psychiatry. 187 (suppl48): 120–124
http://dx.doi.org/10.1192/bjp.187.48.s120
PMid:16055801
Nasarallah H (2003). A review of the effect of atypical antipsychotics on weight. 28(suppl1):83–96
Petty RG (1999). Prolactin and anti psychotic medications: mechanism of action. Schizophr Res 35(suppl): S67–S73
http://dx.doi.org/10.1016/S0920-9964(98)00158-3
Raja M and Azzoni A (1996). Novel antipsychotics and acute dystonic Reactions. International Journal of Neuropsychopharmacology. 4: 393–397
Rang HP, Dale MM, Ritter JM and Flower RJ (2007). Antipsychotics drugs. In: Rang & Dale's Pharmacology. Elservier, London. 6th Edition: 545–556
Reynolds GP, Hill MJ and Kirk SL (2006). The 5–HT2c Receptor and antipsychotic induced weight gain–mechanisms and genetics. 20 (4 suppl): 15–18.
Tandon R (2002). Safety and tolerability: How do newer generation "atypical" antipsychotics compare?. Psychiatric Quarterly. 73(4): 297–311
http://dx.doi.org/10.1023/A:1020464017021
PMid:12418358
Ucok A and Gaebel W (2008). Side effects of atypical antipsychotics: a brief overview. World Psychiatry. 7: 58–62
PMid:18458771 PMCid:PMC2327229



