Advances in Animal and Veterinary Sciences
Research Article
Advances in Animal and Veterinary Sciences 2 (7): 418 – 423Comparison of Effects of Halothane Anaesthesia in Horses with and without Dexmedetomidine Continuous Rate Infusion
Galina Simeonova*, Makram Sleiman
-
Department of Veterinary Surgery, Faculty of Veterinary Medicine, Trakia University, Stara Zagora – 6000, Bularia
*Corresponding author:galinavet@abv.bg
ARTICLE CITATION:
Simeonova G and Sleiman M (2014). Comparison of effects of halothane anaesthesia in horses with and without dexmedetomidine continuous rate infusion. Adv. Anim. Vet. Sci. 2 (7): 418 – 423.
Received: 2014–08–05, Revised: 2014–09–07, Accepted: 2014–09–08
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.aavs/2014/2.7.418.423
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
The purpose of this study was to compare the effects of halothane anaesthesia and partial intravenous anaesthesia (PIVA) using halothane and dexmedetomidine continuous rate infusion (CRI) on respiration and coagulation parameters, and recovery in healthy horses. Six healthy ponies aged between 2 and 7 years, weighing 201 ± 70 kG (mean ± SD) were subjected to either halothane or halothane–dexmedetomidine anaesthesia two weeks apart. Acid–base, blood gase, and coagulation parameters were measured at the beginning and after three hours of anaesthesia. Recovery qualities were compared between groups. The results showed that, the addition of dexmedetomidine by CRI at 1.75 µG kG-1hour-1to halothane anaesthesia slightly reduced halothane requirement for maintenance of surgical anaesthesia but had no effects on the recovery time and quality. PIVA using dexmedetomidine and halothane produced respiratory acidosis similar to halothane anaesthesia alone but with significantly more pronounced hypoxaemia. In contrast to halothane anaesthesia, a combination of halothane with dexmedetomidine caused an activation of coagulation system as detected by elevation in plasma D–dimer levels and thrombin time at 3 hours of duration.
INTRODUCTION
The mortality rate in equine anaesthesia is much greater than in other domestic species. Johnston et al., (2004) reported 1% lethality rate in horses undergoing routine surgeries without systemic illness. In the large investigation (Johnston et al., 2002) comprising of 41 825 cases over 6 year period it was found that the death rate in colic surgeries was much greater (11.7%) than noncolic anaesthetic procedures (0.9%). The main cause for perioperative death was cardiovascular arrest or collapse (33%). The degree of hypercoagulability correlated with nonsurvival and thrombotic complications in colic horses (Prasse et al., 1993; Dukti and White, 2009; Dunkel et al., 2010; Cesarini et al., 2010). We evaluated the probability of the two anaesthetic protocols with respect to coagulation disorders.
Thirty two per cent of fatalities connected to anaesthesia in horses occurred during recovery period. Risk factors also were defined and part of them was strongly related to anaesthetic duration and regimen applied with the greatest risk for inhalation anaesthesia in comparison with total intravenous anaesthesia (Johnston et al., 2002). Harmful effects of inadequate perfusion, hypoxia and acid–base abnormalities accompanying general anaesthesia are likely to be cumulative. Recently, great efforts have been made to find safer protocols. The idea of the partial intravenous anaesthesia (PIVA) is to reduce minimal alveolar concentration (MAC) and thus cardiorespiratory depressing effects of inhalation agents by combining inhalation anaesthesia with CRI of an analgesic agent ( Clarke, 2011).
Dexmedetomidine is a relatively new alpha–2 agonist that is much more selective than others in the group which might permit its application without the unwanted cardiovascular effects from activation of alpha-1receptors (Yazbek–Karam and Aouad, 2006). Administration of dexmedetomidine as an adjunctive agent to general anaesthesia produced an anaesthetic–sparing effects in human (Khan et al., 1999; Fragen and Fitzgerald, 1999). There was also dose–dependent reduction in isoflurane concentration by 35–50%, and lowering sevoflurane requirements by 17%. Similar changes in isoflurane concentrations necessary for maintenance of surgical anaesthesia by CRI of dexmedetomidine were observed also in dogs (Pascoe et al., 2006) and horses ( Marcilla et al., 2012). Medetomidine, whose pharmacologically active dextroisomer is dexmedetomidine, was reported to decrease the MAC of halothane by 90% in dogs (Vickery et al., 1989). In the present study, we tested the effects of dexmedetomidine CRI on halothane requirements for maintenance of surgical anaesthesia as well as on the respiration and recovery in clinically healthy horses. The purpose of the study was to compare the effects of halothane anaesthesia and partial intravenous anaesthesia (PIVA) using halothane and dexmedetomidine on respiration and coagulation parameters and recovery in healthy horses
MATERIAL AND METHODS
The study was performed with a permission given by the Ethical Committee of the Faculty of Veterinary Medicine at Trakia University in Stara Zagora.
Animals
Six healthy horses aged between 2 and 7 years, weighing 201 ± 70 kG (mean ± SD) were included in the experiment. They had been bought from owners and were maintained under similar feeding and managemental conditions for a month. During the adaptation period, an anthelmintic treatment was given using mebendazole 7.5 mG/kG PO (Telmin® paste, Janssen Animal Health, Belgium). All animals were allocated in ASA grade I or II based on preliminary clinical and laboratory investigations.
Horses were assigned first to control/saline (S) group and next (with a gap of two weeks) to experimental/dexmedetomidine (D) group in order to produce cross–over design.
Food was withheld 12 hours before general anaesthesia but water access was not restricted.
Experimental Design
Premedication was identical in the two groups. Acepromazine maleate (Neurotranq®, Alfasan International, Holland) 0.03 mG/kG was given IV. Thirty minutes later two 14–gauge 2.1x50 mm catheters (Venocan plus®, Kruuse, Denmark) were placed in both jugular veins and xylazine hydrochloride (Alfasan International, Holland) 0.8 mG/kG was administered IV.
Anaesthetic induction was also the same in two groups and was induced five to ten minutes after xylazine injection by mixture of ketamine hydrochloride (Anaket®, Richter Pharma, Austria) 2.2 mG/kG with diazepam (Diazepam, Sopharma, Bulgaria) 0.05 mG/kG injected intravenously.
After tracheal intubation (20–22 mm OD tracheal tube, Cook) the horses were restrained on to a surgical table covered with an inflatable mattress and positioned in dorsal recumbency. The tube was connected to a large animal anaesthesia machine LDS 300 (Surgivet, USA) equipped with large animal ventilator DHV 1000 (Surgivet, USA) and out–of–circuit Fluoteck Mark III halothane vaporizer.
Anaesthesia was maintained with halothane (Narcotan®, Zentiva, Check Republic) in oxygen 100% through closed circuit system for 3 hours. As soon as the vaporizer was switched on, group D received a CRI of dexmedetomidine hydrochloride (Dexdomitor®, Orion Pharma, Finland) 1.75 µG kG-1hour-1diluted with saline to a concentration of 0.01 mG ml –1, while group S received a CRI of equivalent volume of saline solution administered by means of microinfusion pump WZ–50C6 (All Pro, China) until the end of anaesthesia. Syringes were prepared in advance so as the anaesthetist was unaware of medications given.
Arterial access was achieved by cannulation of left or right facial artery using 22–gauge 0.9x25 mm catheter (Venocan plus®, Kruuse, Denmark). Arterial blood samples were collected immediately after catheter placement and before the end of anaesthesia for blood gases, electrolytes and acid–base status measurement. Repiratory/blood gases VetStat® cassettes and VetStat® electrolyte and blood gas analyzer (IDEXX Laboratories, Inc., USA) were used for that purpose. Arterial lactate levels were measured by colorimetric method using enzymatic Roche/Hitachi lactate reagent (Roche Diagnostica, Germany). The arterial access was used also for invasive measurement of blood pressure.
Besides systolic, diastolic, and mean arterial blood pressures a patient monitor PM–9000Vet (Mindray, China) was used to record ECGs, heart rate (HR), haemoglobine oxygen saturation (Sat), respiratory rate (RR), inspired and expired fractions of halothane, CO2, O2, and minimal alveolar concentration (MAC) of halothane. For that purpose II lead was used derived from sternal–wither configuration. Saturation probe was placed on the tongue. These parameters were recorded every five minute.
Ringer’s solution (Actavis, Bulgaria) was administered through the second venous catheter in both groups throughout the anaesthesia at a minimal rate of 10 ml kG-1hour-1with some corrections. The rate was adjusted to maintain mean arterial pressure above 60 mmHg. Nevertheless, if blood pressure continued to drop, dopamine hydrochloride (Warsaw Pharmaseutical Works Polfa SA, Poland) was infused starting with a rate of 0.5 µG kG-1minute-1and adjusted as required.
Venous blood samples were taken at the beginning and at the end of anaesthesia in vials containing sodium citrate for measurement of some parameters of coagulation system such as fibrinogen, prothrombin time (PT), activated partial thomboplastin time (APTT), thrombin time (TT) using coagulometer Amelung KC1A (Germany) and tests of Human Diagnostica (Germany). Blood D–dimer was measured by means of quantitative latex–aglutination method (Spinreact, Spain).
The animals were allowed to breathe spontaneously. If the arterial partial pressure of CO2 (PaCO2) increased above 60 mmHg, the arterial partial pressure of O2 (PaO2) decreased bellow 100mmHg, or RR was lower than 4 breaths minute-1for more than 3 minute an intermittent positive pressure ventilation (IPPV) was provided. Tidal volume of 20 ml kG-1, peak inspiratory pressure (PIP) no more 30 cm H2O, RR 8 breaths minute-1, and inspiratory time 2.5 seconds were set in an assisted–controlled mode of respiration. Urinary catheter was placed as well.
The depth of anaesthesia was assessed observing respiration and cardiovascular parameters, ocular position, movements, reflexes and moisture, and deep surgical plane was maintained by altering the inspired halothane concentrations. Nociceptive electrical stimulation was given 30 minutes after induction of anaesthesia and every 30 minutes thereafter. In case of positive reaction to electrical stimulation (gross purposeful movement of non stimulated limbs) or spontaneous movement of the horse without stimulation the halothane concentration was increased. For determination of adequate anaesthetic depth, a constant current (CC) electrical stimulation was used (Levionnois et al., 2009). To deliver CC stimulation, an electrical stimulator Tonus 2M (Drujba Ltd., Vratza, Bulgaria) was used. Two surface electrodes were applied to the shaved and moistured skin over the lateral palmar digital nerve between the coronary band and the fetlock joint of the right hind limb, 1 cm apart and secured with elastic bandage. Stimuli consisted of an interchangeable 1.5 seconds lasting sequence of CC 40 mA semicircle–wave pulses delivered at a frequency of 50 Hz and 1.5 seconds lasting pause for 6 seconds.
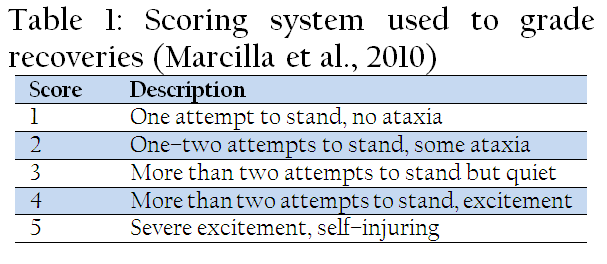
At the end of 3 hours of tracheal intubation, the vaporizer was switched off and the animals were moved to a padded box where they were allowed to recover without assistance, oxygen supplementation, or additional sedation. As soon as the animals were able to swallow, the endotracheal tubes were removed. The quality of recovery was evaluated by recording extubation time, time to sternal and time to standing positions, and observing the number of attempts to stand, the presence of violence, ataxia, or injury. The quality of recovery was scored from 1 to 5 grades (Table 1).
Statistical Analysis
Data were analyzed by means of a commercially available software package (Statistica® 6–0 version, StatSoft Inc. USA). The distribution of continuous data was tested using the Kolmogorov–Smirnov test. Analysis of variance (ANOVA) for repeated measurements was used to detect the influence of time and treatment upon each variable. Recovery scores and durations were compared between two anaesthetic protocols using one–way ANOVA and post–hoc Fisher test. The minimal level of statistical significance was set at 0.05 for all analyses.
RESULTS
In our experiment with horses no significant differences but only tendency were observed between groups S and D in terms of MAC by periods and with time (Table 2). We recorded an 8% decrease MAC as well as 11.1% decrease end tidal halothane concentrations (EtHal) in D group. We also found significantly lower vaporizer settings in D group for maintenance of surgical anaesthesia as well as reduction of inspired and expired halothane concentrations compared to S group with significant difference in several periods. The lowest measured inspired oxygen concentration was 85 % in both groups. With regard to expired CO2 concentrations, lower values were detected in D group.

Table 2: Values (Mean ± SD) of the anaesthesiological parameters of horses subjected to halothane anaesthesia (group S) and combined halothane inhalation with CRI of dexmedetomidine (group D) detected at 10 minute intervals
Pure halothane and combined halothane–dexmedetomidine anaesthesia did not differ significantly in reference to heart rate, respiratory rate, oxygen saturation, mean, and diastolic arterial pressures (Table 3). Only systolic blood pressure was elevated in D group at 100th and 110th min.
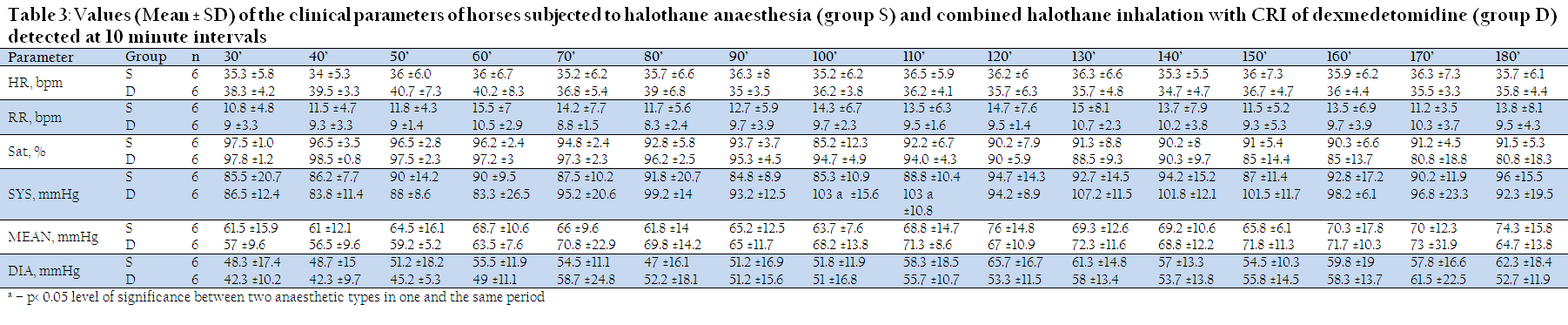
Table 3: Values (Mean ± SD) of the clinical parameters of horses subjected to halothane anaesthesia (group S) and combined halothane inhalation with CRI of dexmedetomidine (group D) detected at 10 minute intervals
Our results showed that 3 hour lasting halothane anaesthesia in horses with or without dexmedetomidine produced respiratory acidosis and hypoxaemia more pronounced in D group (Table 4). Unlike halothane anaesthesia, PIVA with halothane and dexmedetomidine activated coagulation system as TT and D–dimer were enhanced in this group only. Lactate levels were also elevated with this anaesthesia (Table 5).

Table 4: Blood gases and acid–base (BG–AB) parameters of horses (Mean ± SD) subjected to halothane anaesthesia (group S) and combined halothane inhalation with CRI of dexmedetomidine (group D)
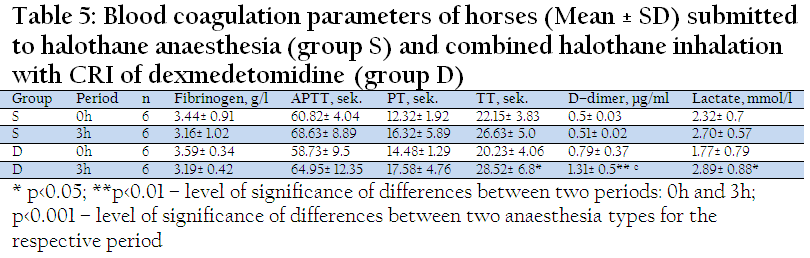
Table 5: Blood coagulation parameters of horses (Mean ± SD) submitted to halothane anaesthesia (group S) and combined halothane inhalation with CRI of dexmedetomidine (group D)
There were no significant differences in the parameters used to assess recovery quality between the two groups (Table 6).

Table 6: Recovery score and times in halothane anaesthetized horses with (group D) and without (group S) a CRI of dexmedetomidine
DISCUSSION
We found out that PIVA with dexmedetomidine decreases slightly halothane requirements to maintain surgical anaesthesia in healthy horses. MAC serves to estimate the potency of anaesthetic agents. However, MAC could be decreased by a number of factors, including decreased body temperature, hypoxia and acidosis, sedative drugs including alpha–2 agonists, systemic and epidural opiates and aging. At the same time, the measurement of end–tidal volatile anaesthetic agent concentration is a standard component of modern anaesthetic monitoring. End tidal concentration provides reliable means to monitor continuous brain concentration of volatile anaesthetics provided adequate time is allowed for equilibration between alveolus, blood and effect site, thus could reliably serve to estimate the depth of anaesthesia.
The halothane–sparing effect of dexmedetomidine was expected to be more pronounced as was reported in other works with rats and dogs (Segal et al., 1989; Rioja et al., 2005; Pascoe et al., 2005; 2006). Aantaa et al., (1997) studied the effects of dexmedetomidine at two different doses in women undergoing abdominal hysterectomy and reported that at higher doses, dexmedetomidine reduced the isoflurane requirement by 47%. However, investigations in horses failed to demonstrate an isoflurane sparing effect of CRIs of romifidine, detomidine or dexmedetomidine (Devisscher et al., 2010; Schauvliege et al., 2011; Marcilla et al., 2012). Rioja et al., (2005) have concluded that dexmedetomidine caused 72% reduction in MAC of halothane and 43% reduction in MAC of isoflurane in rats. The reason for this discrepancy may be connected to the species differences. On the other hand, in another study it has been shown that halothane and isoflurane act at different sites to produce immobility (Santos et al., 2012). In the study of Schmeling et al., (1999) dexmedetomidine produced a differential anesthetic–sparing action on caudal central nervous system cardiovascular control centers (decreased MAC and MACBAR) versus telencephalic indices of anaesthetic depth (MACBS and MACISOELECTRIC). Therefore, the anesthetic–sparing action of alpha–2–adrenergic agonists may be dependent on the site of action at CNS. Another possible explanation for the unsatisfactory halothane–sparing effect of dexmedetomidine could be its low dose used for CRI.
We chose acepromazine and xylazine for premedication and diazepam and ketamine for anaesthetic induction as these agents are considered relatively safe. Acepromazine reduced the risk of death over all the other premedicants, and induction with diazepam and ketamine was not associated with perioperative mortality rate (Johnston et al., 2002). Moreover, their effects were overwhelmed by the effects of inhalation agents during maintenance of anaesthesia. Therefore, the influence of agents used for premedication and induction upon investigated parameters could be neglected and the alterations observed might be attributed to the effects of agents used for maintenance.
Halothane, isoflurane and sevoflurane inhalation anaesthesia in horses produced hypotension and hypercapnia in similar level (Kazuto, 2001). Hypotension observed in several animals in our study was successfully overcome with dopamine infusion. Comparing spontaneous ventilation and IPPV in isoflurane–medetomidine anaesthetized horses for elective surgeries Kalchofner et al., (2009) found similar respiratory acidosis and hypotension. Spontaneous ventilated horses anaesthetized with halothane for elective procedures had significantly higher PaCO2 and P (A–a) O2 (Day et al., 1995).
Dorsal recumbency contributes considerably to the development of hypoxygenation and respiratory acidosis in the horses. We found a significantly lower PaO2 and saturation during halothane–dexmedetomidine anaesthesia in comparison to halothane anaesthesia alone. The same was observed by Marcilla et al., (2012) comparing isoflurane and isoflurane–dexmedetomidine anaesthesia in horses. Hypoxygenation persisted in our experimental animals at all the time intervals inspite of 100% of oxygen application. According to Nyman et al., (1990) horses develop atelectasis in dependant lung regions early during anaesthesia in dorsal recumbency, and that atelectasis is the most likely explanation for the large shunt and impaired arterial oxygenation regularly seen during anaesthesia, especially long–lasting. It is interesting that hypoxaemia was more pronounced in D than in S group. Alpha–2 agents have minimal respiratory depressing effects on their own but probably the use as an adjunct to a volatile anaesthetic may deepen its respiratory depressive properties.
Both halothane and halothane–dexmedetomidine anaeshesia decreased arterial pH. Acidosis was respiratory type as was reported in previous studies (Dinev and Hubenov, 2002), with nonsignificant elevation of PaCO2 after 3 hour of anaesthesia. In group D, blood lactate levels also increased with time, which corresponded to higher anion gap. Base excess decreased in both groups as a sign of metabolic compensation. Lactate increased significantly in D group at 3 hour but there were not any differences between the two anaesthetic regimens for the respective period. This might be due to slightly lower initial levels measured in group D or to more pronounced hypoxaemia.
According to the results of Marcilla et al., (2010), constant rate infusion of dexmedetomidine produced similar cardiovascular effects in isoflurane anaesthetized horses independent of infusion rates used (1 and 1.75 μg kG-1h–1). The second rate was chosen in our experiment and we found that HR did not change significantly with time with and without dexmedetomidine CRI. Systolic arterial pressure was higher in group D at 100 and 110 minute of anaesthesia, but this could be due to dopamine administration. Moreover, dopamine was administered in 3 animals of D group and only 1 animal of S group. We did not observed any arrhythmias in both groups likely because of low halothane concentrations used or acepromazine included in the protocol, as it reduces sensitivity of the myocardium to catecholamines. It is known that IPPV can cause an impairment in circulation. In our study five animals from both groups needed periodical IPPV so the influence of IPPV on cardiovascular parameters could be considered the same with both treatments.
Alsaad and Nori (2009) reported significantly lowered platelet count and fibrinogen and higher PT and APTT in colic horses in comparison with healthy individuals. Coagulopathies in horses with colic seem to be associated with poor outcome. Dinev and Hubenov (2002) reported a shortening of APTT during halothane anaesthesia in horses. Our results showed no difference after 3 hours of halothane anaesthesia either in comparison to the beginning or addition of CRI of dexmedetomidine with respect to fibrinogen levels, PT and APTT. Volatile anaesthetics in a concentration of 1 MAC can reduce the adhesion of platelets in the coronary system under reduced flow conditions (Heindl et al., 1998). This action does not arise from vasodilation or inhibition of ischaemic stress. The adherence was reduced with each 1 MAC isoflurane, sevoflurane or halothane. Volatile anaesthetics at 0.5 MAC did not inhibit platelet adhesion to a statistically significant extent in any case. Elrashidy et al., (2007) also reported an inhibition of platelet aggregation by sevoflurane, whereas isoflurane had neither effect on platelet aggregation nor other coagulation parameters during intra– and postoperative periods.
Halothane anaesthesia did not produce significant alterations in coagulation parameters in our study, whereas the addition of dexmedetomidine CRI led to elevation in TT and D–dimer levels. The interaction of dexmedetomidine with alpha–2 adrenergic receptors on platelets resulted in decreased platelets aggregation (Yazbek–Karam and Aouad, 2006). Coagulation system might be activated during hypoxaema, which was detected after 3 hours, more obvious in D than in S group. Plasma D–dimer concentration is a sensitive test for assessing coagulation system with prognostic meaning and a potential cut–off value for non–survival colic horses was found at around 4000 ng/ml (Cesarini et al., 2010). Halothane–dexmedetomidine anaesthesia produced an elevation in D–dimer values to levels of 1310 ng/ml. So if the horse is close to the cut–off point at admission it is better to avoid this anaesthesia. Coagulation changes observed in our study are probably not due to pharmacological effects of anaesthetic agents but to hypoxaemia.
Better recovery quality in horses was associated with shorter duration of anaesthesia, longer recovery times, less invasive surgery, a lower pulse rate at induction and higher pulse and respiratory rates during anaesthesia (Young and Taylor, 1993). The addition of medetomidine and lidocaine to isoflurane anaesthesia in healthy horses submitted to arthroscopic surgery improved the quality of recovery although with longer duration (Valverde et al., 2010). Hubbell et al., (2011) reported longer than our times to extubation (31 min), to sternal (88 min), and to standing (96 min) during recovery period of three hour lasting isoflurane anaesthesia without CRI. Our results were in concordance with the study of Kazuto (2001) who reported better quality of recovery from halothane than from isoflurane anaesthesia in horses. The same was reported by Warwa et al., (2009). It was also seen that the age over 15 years linearly increase recovery time and score and body mass bellow 250 kG significantly decrease recovery time but without any effect on the score. Anaesthetic did not influence recovery time whereas longer lasting anaesthesia (> 60 min.) was connected with worse recovery quality. Whereas, a dexmedetomidine CRI improved recovery quality in isoflurane anaesthetized horses (Marcilla et al., 2012). In the present study we did not find any differences in recovery time and score after halothane anaesthesia alone or with CRI of dexmedetomidine in healthy horses.
In conclusion, the addition of dexmedetomidine by CRI at 1.75 µG kG-1hour-1to halothane anaesthesia in healthy horses slightly reduced the halothane requirements for maintenance of surgical anaesthesia but had no effects on the recovery time and quality. PIVA using dexmedetomidine and halothane produced respiratory acidosis similar to halothane anaesthesia alone but significantly more pronounced hypoxaemia. In contrast to halothane anaesthesia, a combination of halothane with dexmedetomidine caused also an activation of coagulation system as detected by elevation in plasma D–dimer levels and TT after 3 hours of anaesthetic induction.
We declare that there is not any conflict of interests in the present work.
REFERENCES
Aantaa R, Jaakola ML, Kallio A, Kanto J (1997). Reduction of the minimum alveolar concentration of isoflurane by dexmedetomidine. Anesthesiology. 86: 1055 – 1060.
http://dx.doi.org/10.1097/00000542-199705000-00008
PMid:9158354
Alsaad KM, Nori AA (2009). Equine colic and coagulation disorders. J. Anim. Vet. Adv. 8: 2675 – 2679.
Cesarini C, Monreal L, Armengou L, Delgado MÁ, Ríos J, Jose–Cunilleras E (2010). Association of admission plasma D–dimer concentration with diagnosis and outcome in horses with colic. J. Vet. Intern. Med. 24: 1490 – 1497.
http://dx.doi.org/10.1111/j.1939-1676.2010.0618.x
PMid:20946373
Clarke KW (2011). Total intravenous anaesthesia (TIVA) and partial intravenous anaesthesia (PIVA). In: Proceedings of the 36th World Small Animal Veterinary Congress 14 – 17 October 2011 – Jeju, Korea. 22 – 24.
PMCid:PMC3062585
Day TK, Gaynor JS, Muir III WW, Bednarski RM, Mason DE (1995). Blood gas values during intermittent positive ventilation and spontaneous ventilation in 160 anesthetized horses positioned in lateral or dorsal recumbency. Vet. Surg. 24: 266 – 276.
http://dx.doi.org/10.1111/j.1532-950X.1995.tb01330.x
PMid:7653042
Devisscher L, Schauvliege S, Dewulf J, Gasthuys F (2010). Romifidine as a constant rate infusion in isoflurane anaesthetized horses: a clinical study. Vet. Anaesth. Analg. 37: 425 – 433.
http://dx.doi.org/10.1111/j.1467-2995.2010.00556.x
PMid:20712609
Dinev D, Hubenov H (2002). Acid–base, blood gas and haemocoagulation changes in halothane–anaesthetized horses submitted to abdominal surgery. Bulg. J. Vet. Med. 5(4): 241–251.
Dukti S, White NA (2009). Prognosticating equine colic. Vet. Clin. Equine. 25: 217 – 231.
http://dx.doi.org/10.1016/j.cveq.2009.04.004
PMid:19580935
Dunkel B, Chan DL, Boston R, Monreal L (2010). Association between hypercoagulability and decreased survival in horses with ischemic or inflammatory gastrointestinal disease. J. Vet. Intern. Med. 24: 1467 – 1474.
http://dx.doi.org/10.1111/j.1939-1676.2010.0620.x
PMid:21054544
Elrashidy AA, Abdelrahman RS, Ghaly AM, Elsheikh AM, Elsheikh MM (2007). Effects of sevoflurane and isoflurane on coagulation system: A comparative study. Tanta Med. Sci. J. 2 (1): 142 – 152.
Fragen RJ, Fitzgerald PC (1999). Effects of dexmedetomidine on the minimum alveolar concentration (MAC) of sevoflurane in adults age 55 to 70 years. J. Clin. Anesth. 11: 466 – 470.
http://dx.doi.org/10.1016/S0952-8180(99)00081-1
Heindl B, Becker BF, Zahler S, Conzen PF (1998). Volatile anaesthetics reduce adhesion of blood platelets under low–flow conditions in the coronary system of isolated guinea pig hearts. Acta Anaesthesiol. Scand. 42 (8): 995 – 1003.
http://dx.doi.org/10.1111/j.1399-6576.1998.tb05361.x
PMid:9773146
Hubbell JAE, Aarnes TK, Bednarski RM, Lerche P, Muir WW (2011). Effect of 50% and maximal inspired oxygen concentrations on respiratory variables in isoflurane–anesthetized horses. BMC Vet. Res. 7: 23.
http://dx.doi.org/10.1186/1746-6148-7-23
PMid:21639886 PMCid:PMC3133541
Johnston GM, Eastment JK, Taylor PM, Wood JLN (2004). Is isoflurane safer than halothane in equine anaesthesia? Result from a prospective multicentre randomized controlled trial. Equine Vet. J. 36: 64 – 71.
http://dx.doi.org/10.2746/0425164044864723
PMid:14756374
Johnston GM, Eastment JK, Wood JL, Taylor PM (2002). The confidential enquiry into postoperative equine fatalities (CEPEF): mortality results of phases 1 and 2. Vet. Anaesth. Analg. 29: 159 – 170.
http://dx.doi.org/10.1046/j.1467-2995.2002.00106.x
Kalchofner KS, Picek S, Ringer SK, Jackson M, Hässig M, Bettschart–Wolfensberger R (2009). A study of cardiovascular function under controlled and spontaneous ventilation in isoflurane–medetomidine anaesthetized horses. Vet. Anaesth. Analg. 36 (5): 426 – 435.
http://dx.doi.org/10.1111/j.1467-2995.2009.00477.x
PMid:19709046
Kazuto Y (2001). Oxygen–halothane, isoflurane and sevoflurane inhalation anesthesia in horses. Jpn. J. Vet. Anesth. Surg. 32(1): 1 – 8.
http://dx.doi.org/10.2327/jvas.32.1
Khan ZP, Munday IT, Jones RM, Thornton C, Mant TG, Amit D (1999). Effects of dexmedetomidine on isoflurane requirements in healthy volunteers, 1: Pharmacodynamic and pharmacokinetic interactions. Br. J. Anaesth. 83: 372 – 380.
http://dx.doi.org/10.1093/bja/83.3.372
PMid:10655905
Levionnois OL, Spadavecchia C, Kronen PW, Schatzmann U. (2009). Determination of the minimum alveolar concentration of isoflurane in Shetland ponies using constant current or constant voltage electrical stimulation. Vet. Anaesth. Analg. 36: 9 – 17.
http://dx.doi.org/10.1111/j.1467-2995.2008.00420.x
PMid:19121154
Marcilla MG, Schauvliege D, Duchateau L, Gasthuys F (2010). Cardiopulmonary effects of two constant rate infusions of dexmedetomidine in isoflurane anaesthetizsd ponies. Vet. Anaeth. Analg. 37: 311 – 321.
http://dx.doi.org/10.1111/j.1467-2995.2010.00537.x
PMid:20636563
Marcilla MG, Schauvliege S, Segaert S, Duchateau L, Gasthuys F (2012). Influence of a constant rate infusion of dexmedetomidine on cardiopulmonary function and recovery quality in isoflurane anaesthetized horses. Vet. Anaesth. Analg. 39: 49 – 58.
http://dx.doi.org/10.1111/j.1467-2995.2011.00672.x
PMid:22151875
Nyman G, Funkquist B, Kvart C, Frostell C, Tokics L, Strandberg A, Lundquist H, Lundh B, Brismar B, Hedenstierna G (1990). Atelectasis causes gas exchange impairment in the anaesthetized horse. Equine Vet. J. 22: 317 – 324.
http://dx.doi.org/10.1111/j.2042-3306.1990.tb04280.x
PMid:2226395
Pascoe P (2005). The cardiovascular effects of dexmedetomidine given by contionuous infusion during isoflurane anesthesia in dogs. Vet. Anaesth. Analg. 32: 9.
http://dx.doi.org/10.1111/j.1467-2995.2005.00232a_18.x
Pascoe PJ, Raekallo M, Kuusela E, McKusick B, Granholm M (2006). Changes in the minimum alveolar concentration of isoflurane and some cardiopulmonary measurements during three continuous infusion rates of dexmedetomidine in dogs. Vet. Anaesth. Analg. 33: 97 – 103.
http://dx.doi.org/10.1111/j.1467-2995.2005.00236.x
PMid:16475999
Prasse KW, Topper MJ, Moore JN, Welles EG (1993). Analysis of hemostasis in horses with colic. J. Am. Vet. Med. Assoc. 203 (5): 685 – 693.
PMid:8407538
Rioja E, Santos M, Martínez F, Tendillo F (2005), Dexmedetomidine and midazolam interaction is synergistic with isoflurane and additive with halothane in terms of MAC reduction. Vet. Anaesth. Analg. 32: 10 – 11.
http://dx.doi.org/10.1111/j.1467-2995.2005.00232a_21.x
Santos M, Ibancovichi JA, Millán I, Tendillo FJ (2012). Isoflurane but not halothane minimum alveolar concentration–sparing response of dexmedetomidine is enhanced in rats chronically treated with selective α2–adrenoceptor agonist. Lab. Anim. 46 (3): 215 – 219.
http://dx.doi.org/10.1258/la.2012.011096
PMid:22522415
Schauvliege S, Gonzalo–Marcilla M, Verryken K, Duchateau L, Devisscher L, Gasthuys F (2011). Effects of a constant rate infusion of detomidine on cardiovascular function, isoflurane requirements and recovery quality in horses. Vet. Anaesth. Analg. 38: 544 – 554.
http://dx.doi.org/10.1111/j.1467-2995.2011.00659.x
PMid:21988809
Schmeling WT,Ganjoo P, Staunton M, Drexler C, Neil E. Farber NE (1999). Pretreatment with dexmedetomidine: Altered indices of anesthetic depth for halothane in the neuraxis of cats. Anesth Analg. 88: 625 – 632.
http://dx.doi.org/10.1213/00000539-199903000-00030
http://dx.doi.org/10.1097/00000539-199903000-00030
PMid:10072018
Segal IS, Vickery RG, Maze M (1989). Dexmedetomidine decreases halothane anesthetic requirements in rats. Acta Vet. Scand. Suppl. 85: 55 – 59.
PMid:2571278
Valverde A, Rickey E, Sinclair M, Rioja E, Hathaway A, Cruz A (2010). Comparison of cardiovascular function and quality of recovery in isoflurane–anaesthetized horses administered a constant rate infusion (CRI) of lidocaine or lidocaine and medetomidine during elective surgery. Equine Vet. J. 42 (3): 192 – 199.
http://dx.doi.org/10.1111/j.2042-3306.2010.00027.x
PMid:20486974
Vickery RG, Maze M (1989). Action of the stereoisomers of medetomidine in halothane anaesthetized dogs. Acta. Vet. Scand. Suppl. 85: 71 – 76.
PMid:2571281
Wawra E, Senior JM, Clutton RE, Auer U, Dugdale AHA (2009). Factors influencing the duration and quality of recovery from general anaesthesia in horses: A retrospective study of 590 cases.In: Abstract presented at the 10th World Congress of Veterinary Anaesthesia, 31st August – 4th September, Glasgow, UK. Vet. Anaesth. Analg. 37: 1 – 88.
Yazbek–Karam VG, Aouad MM (2006). Perioperative use of dexmedetomidine. M. E. J. Anesth. 18 (6): 1043 – 1058.
Young SS, Taylor PM (1993). Factors influencing the outcome of equine anaesthesia: a review of 1,314 cases. Equine Vet. J. 25 (2): 147 – 151.
http://dx.doi.org/10.1111/j.2042-3306.1993.tb02926.x
PMid:8467775



