Advances in Animal and Veterinary Sciences
Research Article
Advances in Animal and Veterinary Sciences 2 (5): 296 – 301Comparative Efficacy of Limited Contact–Dynamic Compression Plate and Dynamic Compression Plate for Repair of Diaphyseal Femoral Fracture in Dogs
Farah Ijaz*, Shahla Gull Buk, Muhmmad Arif Khan, Syed Saleem Ahmad, Bilal Haider
-
University of Veterinary and Animal Scienceharis, Lahore, Pakistan
*Corresponding author:drfarah14@gmail.com
ARTICLE CITATION:
Ijaz F, Bukhari SG, Khan MA, Ahmad SS, Haider B (2014). Comparative efficacy of limited contact–dynamic compression plate and dynamic compression plate for repair of diaphyseal femoral fracture in dogs. Adv. Anim. Vet. Sci. 2 (5): 296–301.
Received: 2013–11–29, Revised: 2014–05–13, Accepted: 2014–05–20
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.aavs/2014/2.5.296.301
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
LC–DCP is claimed to be a better implant as compared with the conventional DCP, with respect to low–bone–surface–contact, decreased incidence of porosity, increased and better vascularity of bone tissue, and earlier healing time. In the present study the experimental study was performed on 8– adult dogs divided into 2–groups, A and B. In Groups A and B, DCP and LC–DCP implants were used, respectively. The efficacy of the two plate systems was assessed on the basis of physiological parameters, radio–graphic evaluation. Each dog was radio graphed with medio–lateral projection (ACOMA, JAPAN, Df–50). The radiographs were obtained at an interval of 2 weeks to examine the progress of callus formation with respect to each plate fixation system. Group A showed not good callus formation as some have large callus. Group B dogs showed ideal fixation of implant with accurate Small callus formation. From all this results of this study clearly proved that LC–DCP is better implant than DCP in terms of above parameters for repair of femoral fracture especially in dogs.
INTRODUCTION
The femur is the longest bone in the mammalian skeleton. Femoral shaft fractures can result from high energy as well as low–energy trauma and 30% of patients have multiple injuries in these cases (please give reference to support your statement). Chances of femoral fracture in dogs below 1 year of age are 51.78% and below 2 years of age are 69%. Overall chances of fracture are 29.94% in dogs and most of them are long oblique femoral shaft (73.21%) and supra–condylar fracture (19.64%) (Tercavlioglu, 2009). Fractures can be treated by means of various kinds of external and internal fixation devices. Internal fixation devices include intramedullary pins, elastic stable intramedullary nails (ESIN), bone plates, orthopedic wires, and screws (Roe, 2003). The primary bone plate system is the Dynamic Compression Plate (DCP), in which the holes are designed in such a way that they cause compression of the fracture fragments (Roe, 2003). Their superiority over other implants lies in their characteristics that they can effectively neutralize compression, shearing, rotational and bending forces on the bone (Stiffler, 2004). However despite some advantages, the Dynamic Compression Plates also have some disadvantages such as weakening, osteoporosis and necrosis of the underneath bone. Chances of infection after DCP are generally greater as compared to that after the LC–DCP implants (Perren, 1988). Advantages of LC–DCP over DCP are that it has been designed in such a way that stress is not concentrated at the screw holes. The solid portion of the plate is scalloped at the top and bottom which reduces the area of contact with the bone and hence exerts comparatively less effects on the blood supply (Roe, 2003). The additional benefits of these newer implants are that their torsion and bending properties are comparable with the DCP in the fixation of simple transverse diaphyseal fractures (Miclau et al., 1995).
The present study was designed to evaluate the t two plate fixation systems i.e. DCP plates and LC–DCP plates, in terms of appropriate fracture reduction, implant position, early fracture healing, lesser infection rates, early callus formation and better vascularization of the bone.
MATERIALS AND METHODS
The trial was performed on 8 dogs of local breed of either sex. The dogs were divided into 2 groups, A and B comprising four dogs each. The animals of group A were designated as A1, A2, A3 and A4 and that of group B as B1, B2, B3 and B4.
In group 1, DCP was applied while in group 2, LC–DCP was applied to fix experimentally created long oblique femoral fractures.
Pre–operative dog preparation for surgery: All the dogs were examined for their health status through complete physical examination. All the dogs were kept in kennels of Surgery Section (CMS) of University of Veterinary and Animal Sciences, Lahore. Luke worm water and antibacterial soap Dettol (Lever Broth; Pakistan) were used for bathing. Rabicin vaccine (Rhone Meriux) was administered to all the dogs as a prophylactic measure. Ectoparasites were controlled by using Trichorophan (Seguvon; Symons Pharmaceuticals Pakistan). Fenbendazole was used for control of round worms (Zental suspension; Smith Kline Becham) at the dose rate of 6mg/kg body weight (Green, 2006). The whole limb from the point of hip to the pastern joint was shaved one day before surgery.
In addition to the general surgical instruments, the following special orthopedic instruments were prepared by autoclaving.
Periosteal elevator.
Lowman’s bone clamp.
Bone plates of 2 sizes as follow
Dynamic Compression Plate (DCP) 3.5mm broad
Limited contact–Dynamic compression plate (LC–DCP) 3.5mm broad.
A hand bone drill machine with a set of drill bits of different sizes.
Bone saw.
Plate screws as with specific size 3.5 mm.
Bone hammer.
Depth gauge for 3.5 mm plate
Bone chisel.
A Cerclage wire of 20 gauges.
Lag screws of 30 mm, 32mm, and 34mm length.
Screw driver according to the top of the screw (hexagonal).
Bone tap.
Wire cutter
Wire twister
Anesthetic consideration: The following protocol was followed:
Pre anesthetic medication: Xylazine–HCl at the dose rate of 0.4mg/kg along with atropine sulphate at the 0.02mg/kg body weight before general anesthesia.
Anesthetic medication: Animals were anesthetized with Ketamine–HCl at the doze rate 5mg/kg body in combination with Xylaze, in a ratio of 2:1 was given as a general anesthetic before start of surgery. Half of doze was given at once and the remaining half given in small doses with checking of reflexes after small interval of time as per requirement.
Surgical Protocols
For complete aseptic surgery, sterilized surgical gowns and sterilized disposable surgical gloves, caps, masks were worn before the surgical operation and hands of the surgeon, assistant surgeon and assistants were scrubbed properly with six minutes scrubbing protocol before touching to the sterilized surgical dress (Slatter 2003).
First of all, the operative site was clipped and shaved off at lateral side from point of hip to pastern joint and from medial side also. After clipping and shaving, soap was used to clean surgical site. The dog was moved to the operation theatre and restrained in left lateral recumbence on table. Scrubbing was done in linear fashion from centre towards periphery of complete hind limb to avoid infection by povidone surgical scrub (Pyodine surgical, Brooks). Scrubbing was done to make area free from microbes. Sterile surgical drapes were placed around surgical area and around the lower portion of the limb. The first drape was placed in such a fashion that the central opening area covered the limb and whole body of the animal. Then four drapes fashion was secured to patient skin by towel clamp as the patient’s hind quarter is covered. (Slatter 2003)
All surgical instruments including drapes, scissors, forceps, needle holders, scalpel handles, trays and bowels were sterilized in autoclave before surgery are arranged on the sterilized table after scrubbing of my hands.
Surgical Technique
For the surgery, the animal was placed in lateral recumbence with the limb to be operated on top. The femur was exposed through a cranio–lateral approach (Slatter 2003). Then afterwards, a long oblique fracture was induced using a heck saw. After adequate reduction, the respective bone plates were applied in each group using standard procedures (slatter 2003).
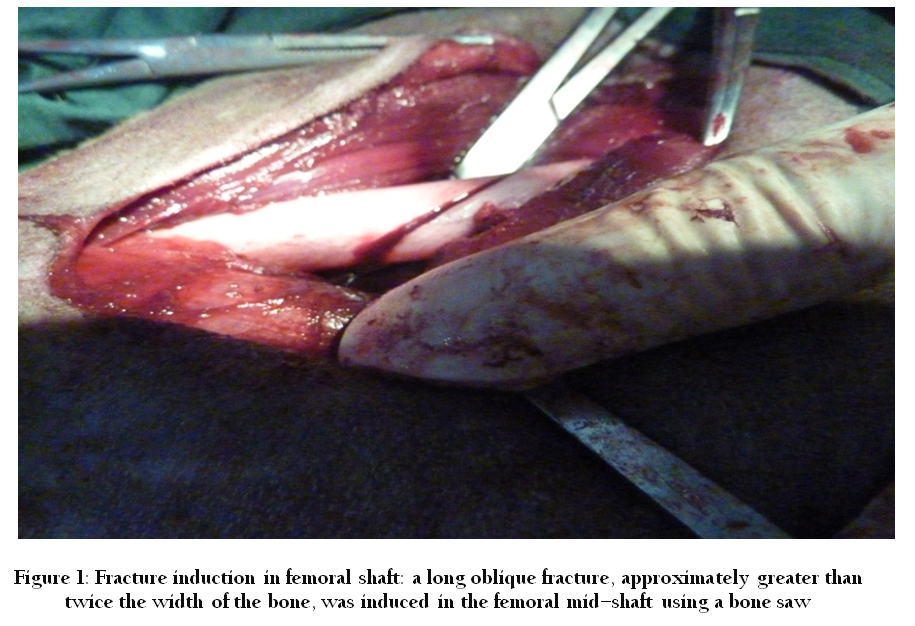
Figure 1: Fracture induction in femoral shaft: a long oblique fracture, approximately greater than twice the width of the bone, was induced in the femoral mid–shaft using a bone saw
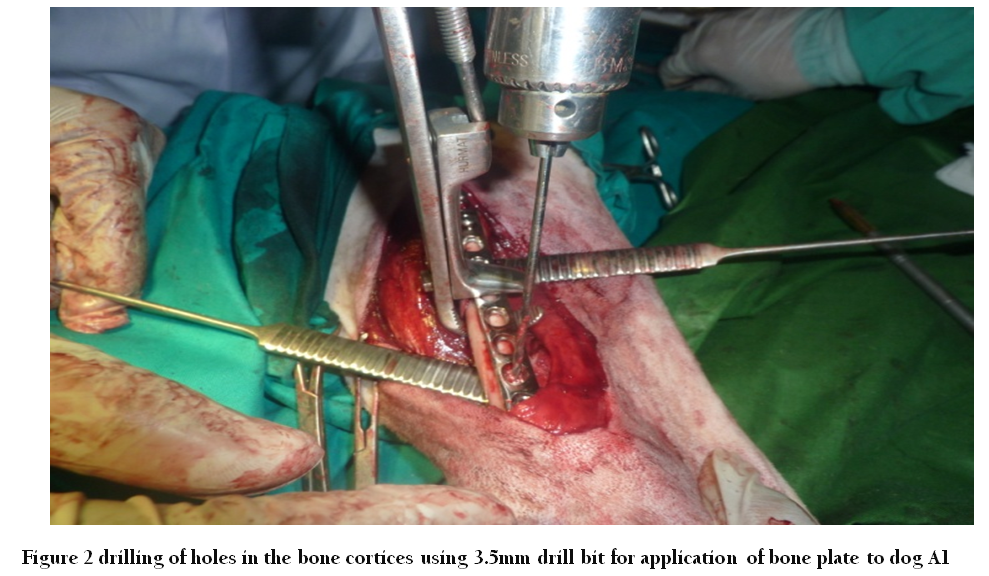
Figure 2: drilling of holes in the bone cortices using 3.5mm drill bit for application of bone plate to dog A1
Observations
The operated animals were kept under observation in animal house facility for the experimental period of three months and the efficacy of the internal implants were evaluated on the basis of the following parameters:
Clinical Evaluation
It included evaluation through the following parameters.
Gait and lameness analysis.
Presence of pain.
Wound healing.
Radiographic Findings
The animals were restrained in lateral recumbence and radiographs of the femora were obtained through a medial–lateral projection. The radiographs were obtained at an interval of 15–days to examine the progress of callus formation with respect to each plate fixation system. The radiographs also made it convenient to visualize the implant position and ascertain proper reduction of the fracture.
REUSLT
In this experimental study my project DCP had been compared with LC–DCP in presence control by keeping physical findings and Radiographic findings.
Experimental Parameters
The effectiveness of the technique was evaluated through following parameters.
Physical findings
Radiographic findings
Physical Findings
Gait and lameness analysis
Presence of pain
Wound healing
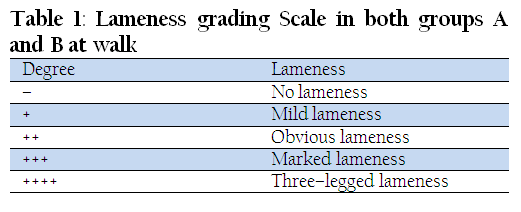
Gait and Lameness Analysis
Animals of each group were tested at various intervals for lameness, according to the grades.
Group A (DCP)
At Walk
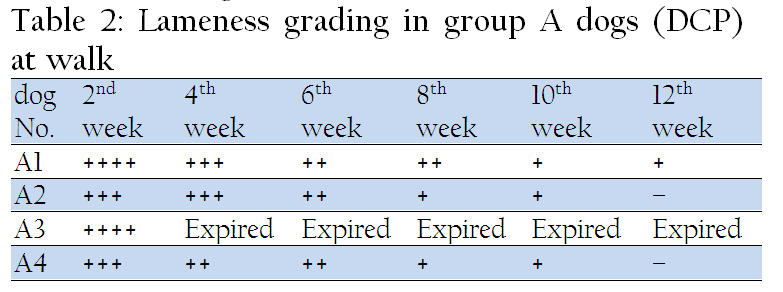
During the healing period, the gait was evaluated on the basis of the degree of lameness. This was checked at an interval of 2 weeks after the surgery till three months post–operatively. The dogs showed different degrees of lameness at different periods.
In the beginning lameness was quite pronounced in all the experimental animals; Dog A1 showed three– legged lameness but with the passage of time it showed improvement and at the end of 12 weeks, no signs of lameness were present. Dog A2 and A4 showed marked lameness even after 2nd week post–operatively, however, at later stages only mild lameness ensued. Dog A3 was weak, lethargic and completely unwilling to stand up post–operatively. At two weeks after the surgery, it developed severe osteomyelitis and signs of 2nd degree lameness. Finally, after the 3rd week it expired.
Further results of lameness are evaluated in Table 2.
At Trot
Animals in group A were also evaluated for lameness at trot, at four weeks postoperatively. The results were not much different from those at walk. Dog A4 showed marked lameness at 2nd week which improved with the passage of time till at 12th week it finally resolved with good recovery and showed no signs of lameness.
Assumption
–union and dog A3 expired in 3rd week
Group B (LC–DCP)
At Walk
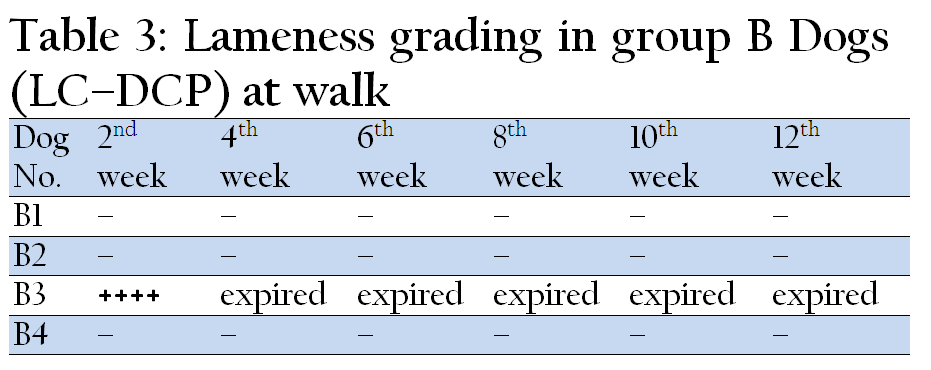
In group B (LC–DCP), during the healing period after the surgical procedure, the gait was evaluated for signs of lameness at walk. This was checked at an interval of 2 weeks after surgery till the end of the experimental period. The results of the LC–DCP were quite promising in all dogs.
Dogs B1, B2 and B4 showed ideal weight–bearing from the very next day after surgery, owing to ideal fixation of the implant. However, dog B3 showed three–legged lameness at 2nd week. Radiographs were suggestive of plate displacement. The plate was removed; however, the dog expired at 2nd week post–operatively due to osteomyelitis and a generalized febrile skin disease.
Further results of lameness are evaluated in Table 3
At Trot
Animals in group B were also evaluated for lameness at trot. This was begun at four weeks post–operatively as in group A. The results were not much different from walk. Dogs B1, B2 and B4 showed good recovery with time, however, Dog B3 showed three–legged lameness at 2nd week due to implant loosening, and later expired at 2nd week post–operatively.
Assumption
From above table it is assumed that lameness is absent in 75% of animals. While in 25% it is sever. This was expired later on due to osteomyelitis.
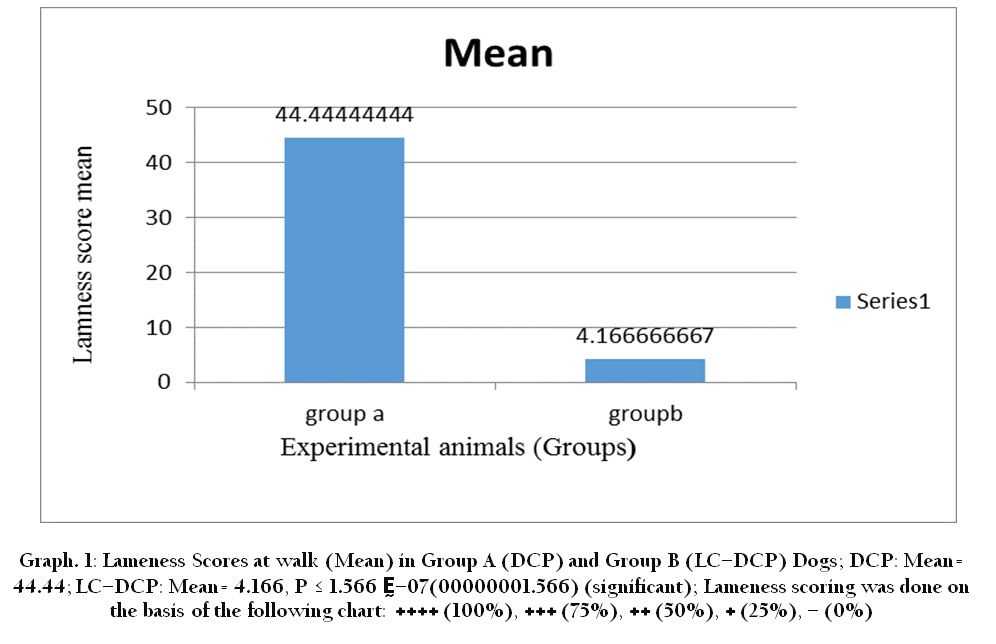
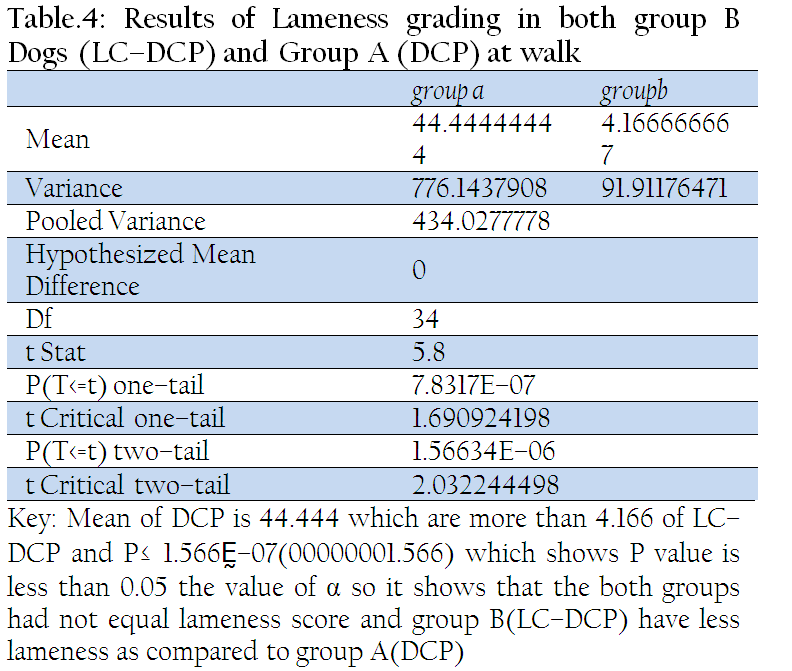
Graph 1: Lameness Scores at walk (Mean) in Group A (DCP) and Group B (LC–DCP) Dogs; DCP: Mean= 44.44; LC–DCP: Mean= 4.166, P ≤ 1.566 Ḛ–07(00000001.566) (significant); Lameness scoring was done on the basis of the following chart: ++++ (100%), +++ (75%), ++ (50%), + (25%), – (0%)
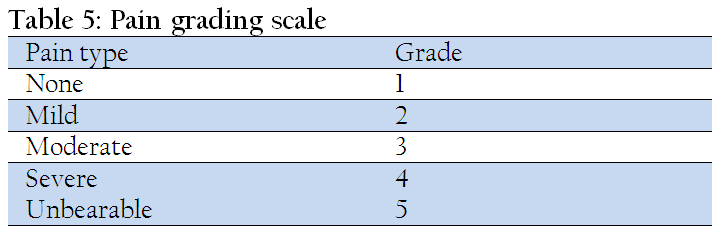
Pain Grading
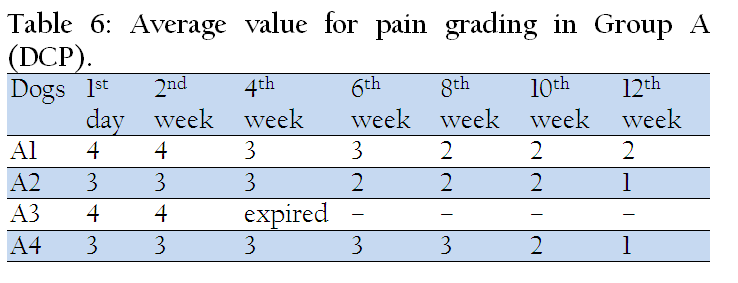
All the dogs showed normal routine without the exhibition of any sever pain signs except dog A1 and A3 in group A (DCP) and B3 in group B (LC–DCP), which showed severe pain on 2nd day postoperatively; however, after the injection of Dicloran®(Diclofenac sodium) BD, the pain was alleviated the very next day. Response to pain was recorded according to the following scale:–
Assumption
From table it is assumed that sever pain in 50 % animals and Moderate in 50% at start. Later on controlled but A1 had pain throughout research trial.
Assumption
From table it is assumed that 75 % have moderate and just 25% sever signs of pain.
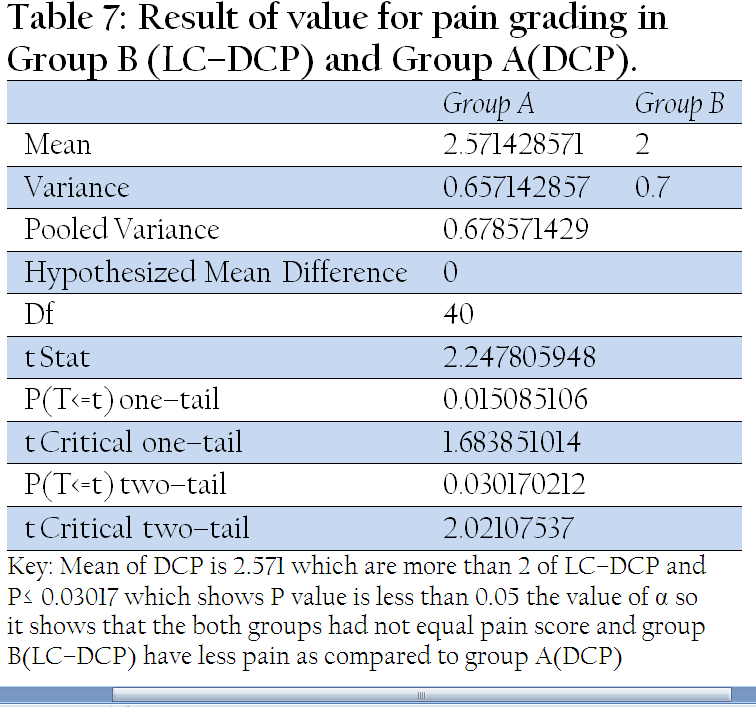
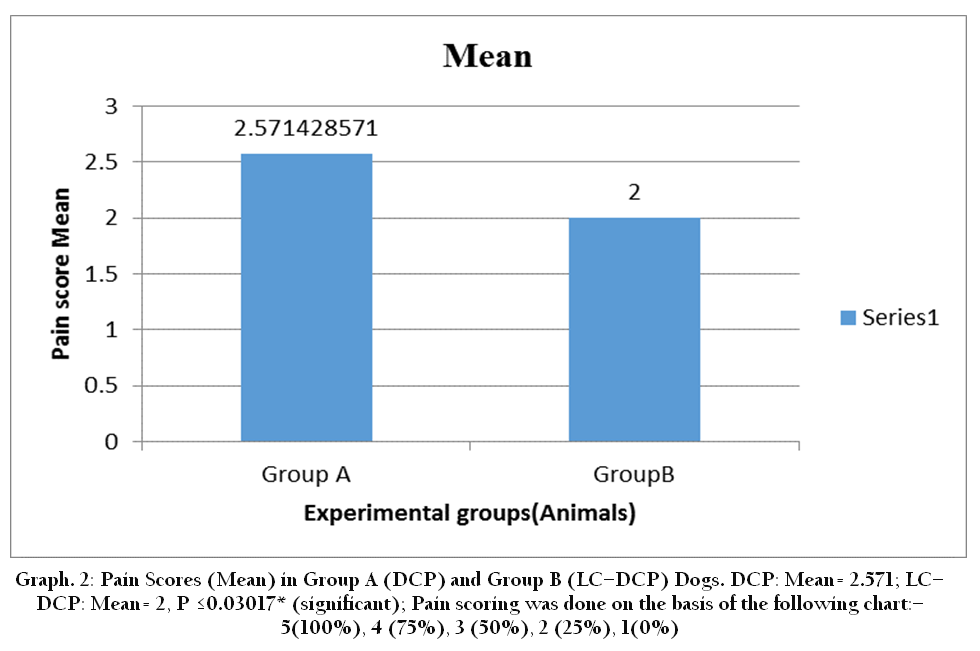
Graph 2: Pain Scores (Mean) in Group A (DCP) and Group B (LC–DCP) Dogs. DCP: Mean= 2.571; LC–DCP: Mean= 2, P ≤0.03017* (significant); Pain scoring was done on the basis of the following chart:–5(100%), 4 (75%), 3 (50%), 2 (25%), 1(0%)
CONCLUSION
From tables No. 4.8 and 4.9 it is concluded that signs of pain were sever in group A (DCP) and in group B (LC–DCP) pain signs were less comparably.
Wound Healing
The wound healing of all dogs took a longer time than normal due to severe weather and temperature fluctuation. On an average, wound healing took about three weeks. Drops of blood were seen falling from the wound incision in dogs A1, A3 of group A and B3 in group B, on the first few days postoperatively. However, this minor bleeding was covered with intramuscular injection of Transamine 250mg/day/dog. Dog No. A3 and B3 expired on 3rd and 2nd week post–operatively while the others remained viable throughout the course without symptoms. While dog A4 in group A and dog B2 in group B in which dehiscence of suture line occurred due to biting and scratching and ultimately led to infection. In these dogs, infection was controlled by using broad–spectrum antibiotics for 5 days Oxidill® 500mg I/V. Daily dressing of the wound was also accompanied using Pyodine® antiseptic lotion (Brookes) and Mycitracin® cream (Galxo Smithkline 2000).

Figure 3: Radiograph of Dog A2 (Group: DCP) – evidence of callus formation at 45 days post–operatively

Figure 4: Radiograph of Dog B1 (Group LC–DCP) – evidence of perfect alignment and fixation of implant, at 2 weeks post–operatively
Radiographic Findings
Each dog was radio graphed. The radiographs were obtained by restraining the animal in lateral recumbence with medio–lateral projection (ACOMA, JAPAN, Df–50). The radiographs were obtained at an interval of 2 weeks to examine the progress of callus formation with respect to each plate fixation system.
Dogs A2 and A4 showed good callus formation. Dog A1 suffered with osteomyelitis in the 3rd week post–operatively; this was covered through optimal treatment, however, due to implant loosening, Dog A1 recovered with a mal–union. Dog A3 expired in the 3rd week post–operatively. Group B dogs showed ideal fixation of implant with displacement occurring only in dog B3 at 2 weeks post–operatively.
DISCUSSION
Orthopedics is an important and advanced part in veterinary surgery and a rapidly expanding field of veterinary practice. Because body movement depends on musculoskeletal system, hence early recovery and return to normal function with minimal complications is the goal of orthopedic major ultimate surgery. In the hind quarter femur is longest and strongest bone in the living beings’ skeleton. Femoral shaft fractures can result from high energy trauma and 30% of patients have multiple injuries in these cases (Flohe, 2009). Chances of femoral fracture in dogs below 1 year of age are 51.78% and below 2 years of age are 69%. Overall chances of fracture are 29.94% in dogs and most of them are long oblique femoral shaft (73.21%) and supra–condylar fractures (19.64%) as documented (Tercavlioglu, 2009). Different techniques have been employed for the purpose of retention like different kinds of bandages, casts, splint bandages, and various kinds of external and internal fixation devices. Internal fixation devices include intra–medullary pins, elastic stable intra–medullary nails (ESIN), bone plates, orthopedic wires, and screws Roe (2003).
The present experiment was conducted to compare two implants and internal fixation of femoral fractures. Their efficacy (DCP & LC–DCP) was evaluated on the basis of lameness at walk and trot, pain scoring and radiographic bases. Both the groups were evaluated and group B (2nd) gave clear indications that LC–DCP resulted in quicker recovery as compared to group A of DCP.
In the present project vital signs as Temperature, Pulse and Respiration were also recorded post–operatively for the check of health status or any infection or stress condition. Elevation in the temperature and pulse of all animals of group A and group B were noted for first few days of postoperative period; similar findings have been reported by Passos (1986), during the early post–operative treatment period after orthopedic surgery.
Group A (DCP) dogs suffered prolonged period of lameness, which were attributed to the complications occurring post–surgically. Fracture union was good in all dogs except dog A1 of group one as it shows mal–union. Mal–union may be due to consequent osteomyelitis (Slatter, 2003), arising as a result of implant loosening, as was the case in Dog A1, as some discussed by Stephan M. Perren (2002). In dog A2 shows marked lameness from beginning, however, later on it was covered. Dog A3 suffered three–legged lameness due to osteomyelitis (Slatter, 2003), consequently leading to its death in the 3rd week post–operatively. Dog A4 shows marked lameness after surgery, however, it later recovered with no signs of lameness. In group B (LC–DCP) the dogs show showed ideal weight bearing from the next day owing to ideal fixation of the implant. Only dog B3 showed three–legged lameness from the 2nd week, the reason being plate displacement. This dog later expired due to osteomyelitis in the 2nd week; these findings were in agreement with those described by Perren (1990).
Pain scoring was almost normal in the first 2 to 3 weeks in all dogs of both groups except dog A1 and A3 who had severe pain. Dog A1 shows signs of osteomyelitis but later on recovered and showed decreased incidence of pain, while Dog A3 expired due to osteomyelitis (Perren, 1990). In group B, dog B3 expired in the 2nd week, post–operatively. The same results have also been evidenced by Perren (1990). All other dogs of group B (LC–DCP) showed moderate pain signs and recovered well with the passage of time and healing process.
Thorough physical evaluation of wounds these animals showed that the healing of surgical site was satisfactory in most of the dogs except dog A1 and A3 in group A, because the both show signs of osteomyelitis, later on the dog A1 recovered but dog A3 expired in the 3rd week. While the dogs in group B showed a positive outcome of the suturing technique, except dog B3 in which dehiscence of suture line occurred due to biting and scratching and ultimately led to infection, which expired in the 2nd week, post–operatively. In these dogs, infection was controlled by using broad–spectrum antibiotics for 7 days Oxidill® 500mg I/V. Daily dressing of the wound was also accompanied using Pyodine® antiseptic lotion (Brookes) and Mycitracin® cream (Galxo Smithkline 2000); and Inj. Pherasym® (Ghazi brothers, Pakistan) as antihistaminic; later the wounds healed by granulation tissue.
The radiographic evaluations of the Dogs A2 and A4 in group A showed large callus formation. Dog A1 suffered with osteomyelitis in the 3rd week post–operatively; this was covered through optimal treatment, however, due to implant loosening, Dog A1 recovered with a mal–union. Dog A3 expired in the 3rd week post–operatively. Contrastingly, in group B, reduction and fixation of the fractured fragments was ideal and dogs regained 100% limb function early on in the healing phase, as evidenced by callus formation and complete bone union. These results were in close agreement with the findings of Bosscha and Snellen (1993). Only Dog B3 showed implant displacement in the 2nd week post–operatively, which ultimately led to osteomyelitis and death of this animal. In all other dogs, the fractured site gained good mechanical strength. This was in accordance with the findings documented by Rand (1981) and Lucas and Peiffer (1999). The radiographic evidence of callus formation was good in group B: LC–DCP shows better results as compared to the DCP group, as also evidenced by Allgower et al. (1969) in their study.
On the basis of the present project it was concluded that the use of Limited Contact–Dynamic Compression Plate (LC–DCP) holds an edge over the conventional Dynamic Compression Plate (DCP). Despite its slightly higher cost, the low degree of plate–bone contact of the LC–DCP promises reduces healing time and optimizes callus formation, leading to early return of limb function, as evidenced through radiography evaluation.
REFERENCES
Arens ST, Hansis M, Schlegal U, Printzen HEG, Ziegler WJ, Perren SM (2000). Infection after open reduction and internal fixation with dynamic compression plates–Clinical and experiment data Anaylsis. Vol. 27, suppl. 3: S – C27 – S – C33.
Bosscha K, Snellen JP (1993). Internal fixation of metacarpal and Phalangeal fracture with AO minifragment screws and plates: a prospective study. Injury 24(3): 166 – 168.
http://dx.doi.org/10.1016/0020-1383(93)90283-C
Feng Z, Li L, He D, Yang C, Qiuk Y (2011). Role of retention of condylar cartilage in open treatment intracapsular condylar fractures in growing goats: three dimentional computed tomographic analysis. Br. J. Oral. Maxillofac. Surg. 50: 523 – 527.
http://dx.doi.org/10.1016/j.bjoms.2011.09.004
PMid:21967705
Filipowicz D, Lanz O, Elder S, Werre S (2009). A biomechanical comparison of 3.5 locking compression plate fixation to 3.5 limited contact dynamic compression plate fixation in a canine cadaveric distal humeral metaphyseal gap model. Vet. Comp. Orthop. Traumatol. 22 (4): 270 –277.
PMid:19597629
Firoozbaksh KK, Moneim E, Pirela–Cruz MA (1993).Comparative fatigue strengths and stabilities of metacarpal internal fixation technique. J. Hand. Surg. [Am]. 18(6): 1059 – 1068.
http://dx.doi.org/10.1016/0363-5023(93)90403-P
Fischer KJ, Provenzano JADA, Tomaino MM (1999). Low–profile versus conventional metacarpal plating system: a comparison of construct stiffness and strength. J. Hand. Surg. [AM]. 24(5)928 – 934.
http://dx.doi.org/10.1053/jhsu.1999.0462
http://dx.doi.org/10.1053/jhsu.1999.0928
PMid:10509270
Gauthier CM, Conrad BP, Lewis DD, Pozzi A (2011). In vitro comparison of stiffness of plate fixation of radii from large– and small–breed dogs. Am. J. Vet. Res. 72(8): 1112 – 1117.
http://dx.doi.org/10.2460/ajvr.72.8.1112
PMid:21801070
Gautier E, Perren SM (1992). Limited Contact Dynamic Compression Plate (LC–DCP) biomechanical research as basis to new plate design. Orthopade. 21 (1): 11 – 23.
PMid:1549332
Grant GR, Olds RB (2003). Treatment of open fractures. Eds, Slatter. Text book of Small Animal Surgery. Philadelphia USA, Pp 1793 – 1797.
Hulse D, Hyman B (2003). Fracture biology and biomechanics. Eds, Slatter. Text Book of Small Animal Surgery, Philadelphia USA, Pp 1785 – 1792.
Jermyn K, Roe SC (2011). Influence of screw insertion order on compression generated by bone plates in a fracture model. Vet. Comp. Orthop. Traumatol. 24(6): 403 – 407.
http://dx.doi.org/10.3415/VCOT-11-06-0081
PMid:21938315
Klauce K, Perren SM (1988). Internal fixation with a self– compressing plate and lag screw: Improvement of plate hole and screw design. I. Mechanical investigation. J. Orthop. Trauma. 5(3):280 – 288.
http://dx.doi.org/10.1097/00005131-199109000-00005
Lazar G, Schulter–Ellis FP (1980). Intramedullary structure of human metacarpals. Hand Surg. [Am]. 5(5); 477 – 481.
http://dx.doi.org/10.1016/S0363-5023(80)80079-7
Lögters T, Windolf J, Flohé P (2009). Femoral shaft fractures. The trauma surgeon journal of the German Society of Trauma Surgery© Springer–Verlag 200910 .1007 / s00113 – 009 – 1669
Lucas GL, Pfeiffer CM (1989). Osteotomy of the metacarpal and phalanges stabilized by AO plates and screws. Ann. Chir. Main. 8 (1): 30 – 38.
http://dx.doi.org/10.1016/S0753-9053(89)80042-0
Perren ZM, Klaue K, Pohler O, Predieri M, Steinemann S, Gautier E (1990). The limited–contact dynamic compression plate (LC–DCP). Arch. Orthop. Trauma. 9(6): 304 – 310.
http://dx.doi.org/10.1007/BF00636166
Rand JA, An KN, Chao EY, Kelly PJ (1981). A comparison of the effect of intramedullary nailing and compression plate fixation on fracture site blood flow and fracture union. J. Bone Joint Surg. Am.63 (3):427 – 442.
PMid:7204443
Risselada M, Bree HV, Kramer M, Rooster HD, Taeymans O, Verleyene P (2005). Ultrasonographic and radiographic assessment of uncomplicated secondary fracture healing of long bones in dogs and cats. Vet. Surg. 34(2): 99 – 107.
http://dx.doi.org/10.1111/j.1532-950X.2005.00017.x
PMid:15860099
Risselada M, Bree HB, Kramer M, Duchateau L, Verleyen P, Saunders JH (2007). Ultrasonographic assessment of fracture healing after plate osteosynthesis. . Vet. Radiol. Ultrasound. 48(4): 368 – 372.
http://dx.doi.org/10.1111/j.1740-8261.2007.00258.x
PMid:17691638
Roe S (2003). Internal fracture fixation. Eds, Slatter. Text book of Small Animal Surgery. Philadelphia USA. Pp 1798 – 1802.
Stephan M, Perren (2002). Evolution of the internal fixation of long bone fractures. J. Bone surg. 84–B: 1093 – 1110.
Stiffler KS (2004). Internal fracture fixation. Clin Tech Small Anim Pract. 19 (3): 105 – 113.
http://dx.doi.org/10.1053/j.ctsap.2004.09.002
PMid:15712456
Tercanlioglu H, Sarieler M (2009). Lucrari Stiintifice Medicina Veterinar. Vol XLII. 2. Pp 98 ¬– 101.



