Journal of Infection and Molecular Biology
Case Report
Journal of Infection and Molecular Biology. 1 (3): 49 – 51Nodular Vasculitis Caused by Chlamydophila pneumoniae
Abdul Majid1*, Nadia Jabeen1, Muhammad Junaid1, Javed Muhammad2, Junaid Ali Shah1, Muhammad Amjid Ali1, Zakir Ullah1, Imran Zamin1, Ali Ahamd Sheikh2
- Department of Microbiology, Hazara University, Mansehra Pakistan
- University Diagnostic Laboratory, University of Veterinary and Animal Sciences, Lahore, Pakistan
*Corresponding author:microbiologistic99@yahoo.com
ARTICLE CITATION:
Majid A, Jabeen N, Muhammad J, Junaid M, Shah JA, Ali MA, UllahZ, Zamin I and Sheikh AA (2013). Nodular vasculitis caused by chlamydophila pneumoniae. J. Inf. Mol. Biol.. 1 (3): 49 – 51.
Received: 201 3–0 7–15, Revised: 2013–08–16, Accepted: 2013–08–23
The electronic version of this article is the complete one and can be found online at
(
http://nexusacademicpublishers.com/table_contents_detail/2/95/html
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Erythema nodosum, a common type of Panniculitis, may develop due to variety of primary infectious or else antigenic stimuli. Nodular vasculitis is a related but definitely different in clinicopathologic reaction pattern of the subcutaneous fat. Current report explains history of a 22–year old Pakistani female patient who developed nodular vasculitis, induced by Chlamydophila pneumoniae. She developed cutaneous vasculitis with onset of respiratory symptoms. The patient is diagnosed with pneumonia, interstitial shadow and thorough shadow on chest CT. Diagnosis was based on clinical signs and changes in antibody titers indicating involvement of C. pneumoniae. Treatment with cephems was unproductive, whereas the newer quinolones were found effective. Following antibiotic administration, nodular vasculitis was subsided along with improvement of the pneumonia. Since this infection is very common, although this term use often asymptomatic, but it must be considered as systematically for the causative agent of nodular vasculitis. To the best of our knowledge, this is the first reported case on nodular vasculitis in Pakistan.
Panniculitis considered as the most common type of Erythema nodosum and may causes by variety of primary infectious or else antigenic stimuli. Nodular vasculitis is different from clinicopathologic reaction pattern of the subcutaneous fat. Literature survey showed that C. pneumonia infection could be involved in the pathogenesis of glomerulonephritis, reactive arthritis, and adult onset of Still’s disease (Fujita et al., 2009).The pathogenesis mechanism of C. pneumonia in systemic disease is not well defined. Regarded to the molecular impressions that is characteristically caused by an antigenic stimulus from Mycobacterium tuberculosis but may be linked with more than a few other primary disorders (Blank et al., 2007). To our familiarity, there are only a few preceding case reports of manifestations of nodular vasculitis in connection with Chlamydophila pneumoniae infection.
A 22–year Pakistani female suffered from skin eruption on her extremities that she first noticed one month before to her access to DHQ hospital, Mardan. A week after the appearance of the eruptions, she developed generalized malaise and a further week after that, she developed fever. She was diagnosed as having fungal infection in DHQ hospital, Mardan and treated with antifungal agents (Amphotericin B for about 10 days) however, effectiveness of these drugs was not observed. Her further medical history was included up on admission as body temperature was 37.4°C, blood pressure was 121/85 mm Hg, and pulse rate was 109 beats/min.
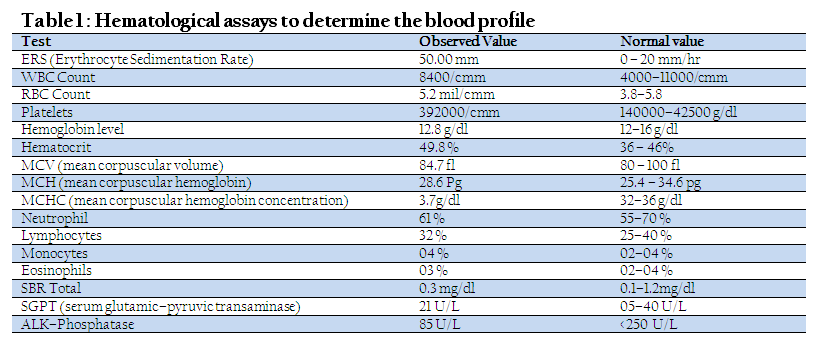
On first day, hematological studies showed that her Erythrocyte Sedimentation Rate (ESR) was 50.00 mm in 1st hr. Units, her G–6–PD Enzyme not Deficient the depolarization time was given 15 Min. Immnuochromotographic test (ICT) for TB was negative. The patient was tested for some test in order to diagnose properly and results are given in Table.
Normally urine color was pale yellow, its specific gravity was 1016, Acidic, no protein, no sugar, WBCs were 2–3/HPF present and Epithelial Cell were a few. In Urine Legionella and Streptococcus pneumonia antigen were negative. Serum Mycoplasma antibody was found negative through complement–fixation test. Anti–C. Pneumoniae IgA was noted as 1.61 C.O.I. (negative <0.80) while anti–C. Pneumoniae IgG 2.82 C.O.I. (positive <1.19). Bleeding time and clotting time was found as 5.0 min and 8.0 min respectively. Chest computed tomography (CT) showed interstitial pneumonia and alveolar pneumonia was intermingled. Physical examination showed violaceous nodules on her extremities and their sizes ranged from 5 to 8 mm in diameter. Biopsy was taken from discharging wound at ankle joint and after histochemical Stain (Ziehl–Neelsen) result was noted negative for acid fast bacilli and PAS/GMS in which Fugal hyphae are not seen. On skin vasculitis, ulceration, granulation tissue formation and focal granulomatous reaction with no evidence of malignancy was observed. No immunoglobulin deposition was shown on direct immunofluorescent studies. She was diagnosed with C. pneumonia infectivity, and this infection induced nodular vasculitis. From 4th to 15th day, she was treated with pazufloxacin/Ciprofloxacin, 1 g daily. The serum CRP fell gradually to become 0.57 mg/dl on the 18th day, and return to normal range by one month. After the 24th day, the indurate erythema began to improve, and seemed to run parallel with the improvement of the serum CRP. Serum CRP was measured again after 40 days after the first time: anti–C. pneumonia IgA 0.90 C.O.I and anti–C. pneumonia IgG 3.18 C.O.I.

Literature survey showed that C. pneumonia infection could involve in the pathogenesis of glomerulonephritis, reactive arthritis, and adult onset of Still’s disease (Fujita et al., 2009). C. pneumoniae antigen might cross–react with several body tissues/organ such as the kidney, blood vessels, skin, joint, and muscle. Immune responses and/or antibodies against it are unknown. On the other hand, C. pneumonia can survive and replicate inside the macrophages, neutrophil, and epithelial cells. Infected cells by C. pneumoniae may then trigger abnormal signal transduction, follow–on in changes of the cytokine profiles and activation and deactivation of certain immunocytes such as macrophages, T cells, B cells, and NK cells (Herrath et al., 2003). Nodular vasculitis has been related with infectious tuberculosis and non–tuberculosis and noninfectious disorders. Infectious non–tuberculosis cases have been related with Nocardia, Fusarium, and Pseudomonas (Patterson et al., 1989). Hepatitis B virus and hepatitis C virus may also be an association with it (Sequra et al., 2008). Previous episodes of superficial thrombophlebitis of the lower legs, hypothyroidism, chronic lymphocytic leukemia, rheumatoid arthritis, and Crohn’s disease are non–infectious associations (Sequra et al., 2008). According to the (Kousa et al., 1980; Erntell et al., 1989; Gran et al., 1993 and Cascina et al., 2002) who diagnosed male and female both patients with respiratory problem using compliment fixation test and micro–immunflourescence test. Some of these patients were reported with associated diseases of Episcleritis, Myocarditis, arthritis, Hepatitis, iritis, Lofgren’s syndrome and conjunctivitis. The results of histology of these patients were found similar as vasculitis to current study and same causative agent C. pneumoniae are of the erythema nodosum nature. On the other hand, the histopathological findings in 3 of the 7 exanthema cases have been reported previously, and these 3 cases showed skin texture of vasculitis (Kousa et al., 1980; Cascina et al., 2002; Bergler–Czop et al., 2009). It is therefore possible that the eruption reported cases as erythema nodosum is actually nodular vasculitis.
To the best of our knowledge, this is the first reported case on nodular vasculitis in Pakistan. The patient showed the signs and symptoms of pneumonia with an interstitial shadow and thorough shadow on chest CT. Cephems were unproductive, whereas the newer quinolones were effective. Changes in the blood antibody titers in addition to these observations and results suggested that this infection is C. pneumoniae. Following antibiotic administration, Nodular vasculitis subsided along with improvement of the pneumonia, suggesting that its causative agent was C. pneumoniae.
REFERENCES
BerglerCzop B, LisSwiety A, Kaminska WG and Brzezinski WL (2009). Erythema nodosum caused by ascariasis and Chlamydophila pneumoniae pulmonary infection – a case report. FEMS Immunol. Med. Microbiol. 57: 236 – 238.
http://dx.doi.org/10.1111/j.1574-695X.2009.00603.x
PMid:19780821
Blank M, Barzilai O and Shoenfeld Y (2007). Molecular mimicry and auto–immunity. Clin. Rev. Allergy Immunol. 32: 111 – 118.
http://dx.doi.org/10.1007/BF02686087
PMid:17426366
Cascina A, MaroneBianco A, Mangiarotti P, Montecucco CM and Meloni F (2002). Cutaneous vasculitis and reactive arthritis following respiratory infection due to Chlamydia pneumoniae: report of a case. Clin. Exp.Rheumatol.20: 845 – 847.
PMid:12508779
Erntell M, Ljunggren K, Gadd T and Persson K (1989). Erythema nodosum – a manifestation of Chlamydia pneumoniae(strain TWAR) infection. Scand. J. Infect. Dis.21: 693 – 696.
http://dx.doi.org/10.3109/00365548909021699
PMid:2694350
Fujita M, Hatachi S and Yagita M (2009). Acute Chlamydia pneumonia infection in the pathogenesis of autoimmune diseases.Lupus.18:164 – 168.
http://dx.doi.org/10.1177/0961203308096069
PMid:19151119
Gran JT, Hjetland R and Andreassen AH (1993). Pneumonia, myocarditis and reactive arthritis due to Chlamydia pneumoniae. Scand. J. Rheumatol.22: 43 – 44.
http://dx.doi.org/10.3109/03009749309095111
PMid:8434247
Kousa M, Saikku P and Kanerva L (1980). Erythema nodosum in chlamydial infections. Acta. Dermatovener (Stockholm).60: 319 – 322.
Marie I, Lecomte F, Levesque H, Janvresse C, Kerleau M, Cailleux N and Courtois H (1999). Lofgren's syndrome as the first manifestation of acute infection due to Chlamydia pneumoniae: a prospective study. Clin. Infect. Dis.28: 691 – 692.
http://dx.doi.org/10.1086/517223
PMid:10194106
Patterson JW, Brown PC and Broecker AH (1989). Infection–induced Panniculitis. J.Cutan.Pathol.16:183 – 193.
http://dx.doi.org/10.1111/j.1600-0560.1989.tb00038.x
PMid:2794161
Sakuma H, Niiyama S, Amoh Y and Katsuoka K (2011). Chlamydophila pneumoniae Infection Induced Nodular Vasculitis – a case report. Case. Rep.Dermatol.3: 263 – 267
http://dx.doi.org/10.1159/000335377
PMid:22220148 PMCid:PMC3250671
Sequra S, Pujol RM, Trindade F and Requena L (2008). Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J. Am. Acad. Dermatol. 59: 839 – 851.
http://dx.doi.org/10.1016/j.jaad.2008.07.030
PMid:19119100
Sundelof B, Gnarpe H and Gnarpe J (1993). An unusual manifestation of Chlamydia pneumoniae infection: meningitis, hepatitis, iritis and atypical erythema nodosum. Scand. J. Infect. Dis. 25: 259 – 261.
http://dx.doi.org/10.3109/00365549309008494
PMid:8511521
Von Herrath MG, Fujinami RS and Whitton JL (2003). Microorganisms and autoimmunity: making the barren field fertile. Nat. Rev.Microbiol.1:151 – 157.
http://dx.doi.org/10.1038/nrmicro754
PMid:15035044



