Journal of Infection and Molecular Biology
Research Article
Journal of Infection and Molecular Biology 2 (2): 19 - 21Prevalence of Brucellosis among the Hospital Patients of Peshawar, Khyber Pakhtunkhwa
Muhammad Shahid1, Abdul Basit2*, Mirza Ali Khan1
- Microbiology and Biotechnology Center, Veterinary Research Institute (VRI), Khyber PakhtunKhwa, Peshawar, 25000, Pakistan
- Department of Microbiology, Kohat University of Science and Technology (KUST), Khyber PakhtunKhwa, 26000, Pakistan
*Corresponding author:aabdul.9090@gmail.com
ARTICLE CITATION:
Shahid M, Basit A, Khan MA (2014). Prevalence of brucellosis among the hospital patients of Peshawar, Khyber PakhtunKhwa. J. Inf. Mol. Biol. 2 (2): 19 - 21
Received: 2014–03–01, Revised: 2014–03–10, Accepted: 2014–03–11
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/jimb.2307-5465/2.2.19.21
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Brucellosis is an occupational disease with those predominantly at risk either having close contact with livestock or handling them. In developing countries this disease has a public health significance as well as animals and economic implications for communities. The objective of the present study was to estimate the brucella infection among hospital patients in district Peshawar, Khyber PakhtunKhwa. A total of 678 blood samples were collected from patients originating from different hospitals located in Peshawar, over the period of three years (2009 – 2011). The blood samples were screened for brucellosis on the basis of serum plate agglutination test (SPAT). From the different occupational groups including farmer, livestock owners, employees and other patients, the prevalence of brucellosis was found to be 32.90%, 32.67%, 29.20% and 27.04%, respectively. Moreover higher prevalence of brucellosis was found in female patients (37.06%) and in the patients with age group of 41–60 years (35.06 %). In conclusion brucellosis is an important public health problem in and around district Peshawar. This disease can be prevented especially in rural areas through use of precautionary measure. It is recommended that public health authorities should educate the general public regarding prevention of the brucellosis.
INTRODUCTION
Brucellosis is a zoonotic disease worldwide, especially in the in Asian, Middle East, Central and South American countries (Yohannes et al., 2012). This disease has an important public health problem in many developing countries. World Health Organization figures put the number of new cases of brucellosis more than 500,000 per year (Saeed et al., 2013).
Brucellosis frequently presents in peoples who are in direct contact with infected animals and it’s by products. It is mostly transmitted by consumption of raw milk or unpasteurized dairy products from infected animals (Nielsen and Duncan, 1990). It can also be transmitted to humans via inhalation of aerosolized secretions or by direct contact with infected animal secretions (Lapaque et al., 2006)
Brucellosis in human is septicemic with sudden or insidious onset and is accompanied by continuous fever or undulant fever, joints pain, profuse sweating, nocturnal sweating, weakness, fatigue, headache, irritability, loss of appetite, chest pain and abdominal pain (Doerr, 2012). The duration of the disease may be few weeks or months to several years (Imad et al., 2011).
The clinical presentation of brucellosis is nonspecific and show great variability (Ohtsuki et al., 2008). Diagnosis of this disease, therefore, requires microbiological confirmation by means of the isolation of the bacteria or demonstration by serological tests for the presence of specific antibodies. A large number of different tests have been used for the serological diagnosis of brucellosis, thus demonstrating the lack of an ideal technique (Ruiz-Mesa et al., 2005). The sensitivities of the serological tests for brucellosis range from 65 to 95%, but their specificities are low in areas where brucellosis is endemic because of the high prevalence of antibodies in populations (Ariza et al., 1992). Furthermore, most serological tests can produce cross–reactions with other bacteria (Queipo et al., 1997) and also exhibit important limitations with samples taken from patients with a recent history of brucellosis, in the early phases of the disease, from patients who relapse and from persons exposed professionally (Ariza et al., 1992)
In Pakistan, brucellosis is still remaining one of the major disease problems that affect humans. It has been estimated that prevalence of brucellosis in Pakistan is about 70% (Mohmand et al., 2012). The present study was carried out to estimate the sero–prevalence of brucellosis in hospital patients of District Peshawar.
MATERIALSAND METHODS
Collection of Samples
From 2009 to 2011, a total 678 blood samples were collected from patients referred by Leady Reading hospital (LRH), Khyber Teaching Hospital (KTH) and other private hospitals in district Peshawar of Khyber PakhtunKhwa, Pakistan. Individual information on sex, age and occupation were obtained by interviewing the patients. The occupational group of patients was comprised on 155 dairy farmers, 101 professions of livestock and 226 Government employees and 196 other patients.
Serum Plate Agglutination Test (SPAT)
The serum samples from patients were subjected to SPAT for screening brucella antibodies as described by Alton et al (1975). The results of agglutination in SPAT were recorded. A titer of 1:80 or above was considered positive for brucellosis according to the instruction of the antigen manufacturer (Global invitro.LLP Sudbury Hill, London UK).
Statistical Analysis
Statistical analysis was performed by using SPSS (version 16.0) software. Significance of difference was determined by using chi square test. Value of p < 0.05 considered as statistically significant.
RESULTS
The sero-prevalence of brucellosis among 155 farmer patients, a total of 51(32.90%) were found positive for brucellosis in which 7/51(13.7%) and 5/51(9.8%) were positive for B. melitensis and B. abortus respectively, the rest of 39 patients were positive on both B. melitensis and B. abortus (Table 1).
Similarly, in 101 profession of livestock farmer patients, 33(32.67%) were found positive for brucellosis, among them 9/33 (27.2%) were positive to B. abortus and 9/33(27.2%) were positive to B. melitensis, the rest of 15 patients were found positive to both B. abortus and B. melitensis (Table 1).
Moreover in 226 government employee patients, a total 66 (29.20%) patients having Brucellosis in which 11 and 10 were found positive to B. abortus and B. melitensis respectively. Remaining 45 were positive for both species of brucella (Table 1). In 196 other patients, 53(27.04%) were found positive for brucellosis, in which 8 and 11 were positive for B. abortus and B. melitensis respectively, whereas 34 were found positive for both B. abortus and B. melitensis (Table 1).
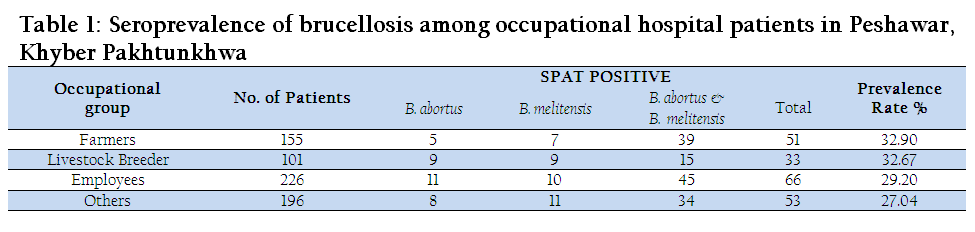
Table 1: Seroprevalence of brucellosis among occupational hospital patients in Peshawar, Khyber Pakhtunkhwa
In the present study higher prevalence of brucellosis was estimated in females (37.06%) followed by males (24.2%) (Figure1).
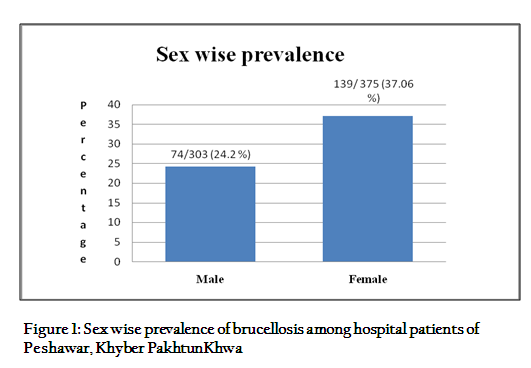
Figure 1: Sex wise prevalence of brucellosis among hospital patients of Peshawar, Khyber PakhtunKhwa
A total of 260 patients had age group ranging from 0–20, 21–40, 41–60, and >60 were analyzed for brucellosis, in which 76/260 (29.2%), 106/307(34.5%), 27/77(35.06 %) and 4/34 (1.8 %) respectively were positive for brucellosis. Significant association was found among the different age groups (p< 0.05) (Table 2).

DISCUSSION
Brucellosis is a zoonotic disease world wide. It is the major health problem especially in developing country like Pakistan. Clinical presentation of the brucellosis is nonspecific, and may be very atypical; therefore, laboratory confirmation by isolation or detection of specific anti–brucella antibodies is essential for confirmation of the diagnosis (Rabab et al., 2000).
In the present study farmers, livestock breeders, employees and other patients were screened for brucellosis, which showed 32.90%, 32.67%, 29.2% and 27.04% positive for brucellosis. Mrunalini et al. (2004) in their study reported the prevalence of brucellosis in veterinarians (25.24%), para-veterinarians (23.3), farmers (12.62%), shepherds (11.65%) and other occupational groups (6.8%). In another study Omer et al. (2002) reported the highest prevalence 7.1% among dairy farm workers followed by 4.5% in veterinary personnel. In the present study higher prevalence of brucellosis was recorded, it might be due to fact that only symptomatic patients having febrile illness with joints pain were screened for brucellosis. Furthermore some risk factors for brucellosis were also estimated while getting the information from the patients. The risk factors included the consumption of unpasteurized dairy milk, most of the patients belonged to the rural areas and some of them were totally dependent on livestock so they had more contact with their animals, this could be the main reasons for higher prevalence of brucellosis among them.
In present study higher prevalence of brucellosis were recorded in females 37% followed by male 24.2%. These findings are in agreement with the findings of Din et al (2013), reported the higher prevalence of brucellosis in females i.e. 9.33% followed by 5.33% in males. Similar results were also reported by Riaz (2006) and Azhar et al. (2009) in their study regarding the high prevalence of brucellosis in females. Female housekeepers in rural areas mostly have direct contact with their animals because of daily activities and even some times they attempt to help animals to born and remove aborted fetus from their wombs by hand or without usage of any precaution measures.
In the present study the prevalence of brucellosis in age groupof41–60 year was found higher followed by rest of the age groups. The findings of the present study were somehow similar with study of Mukhtar (2010) and Abo–Shehada et al. (1996), that the age group of 51–60 years had the maximum sero positivity. As brucellosis is an occupational disease, therefore the individuals of this age group might be a greater risk because of prolonged exposure or due to increase activities with regards to their occupations that enhance the risk of gaining infections.
Therefore, further investigation is needed in order to know the exact epidemiological distribution of brucellosis in Peshawar district and to set plan for control and prevention. The public should be made aware of the zoonotic and economic importance of this disease through veterinary extension education and possible resources like media.
REFERENCES
Abo–Shehada MN, Odeh JS, Abu–Essud M, Abuharfeil N (1996). Seroprevalence of brucellosis among high risk people in northern Jordan. Int. J. Epidemiol. 25: 450 –454.
http://dx.doi.org/10.1093/ije/25.2.450
PMid:9119573
Alton GG, Jones LM, Pietz DE (1975). Laboratory techniques in brucellosis.In:World Health Organization Monograph Series Nº 55, Geneva, Switzerland. Volume 2: 1 – 163.
Ariza J, Pellicer T, Pallares R, Foz A, Gudiol F (1992). Specific antibody profile in human brucellosis. Clin. Infect. Dis. 14: 131 – 140.
http://dx.doi.org/10.1093/clinids/14.1.131
PMid:1571417
Azhar K, Rabbani M, Muhammad K, Maqbool A, Shabbir MZ (2009). Seroprevalence of brucellosis in buffalo and human in Swat Valley, NWFP, Pakistan. Pak. J. Zool. 9: 111 – 114.
Din AMU, Khan SA, Ahmad I, Rind R, Hussain T, Shahid M, Ahmed S (2013). A study on the seroprevalence of brucellosis in human and goat populations of district Bhimber, Azad Jammu and Kashmir. J. Anim. Plant Sci. 23: 113 – 118.
Imad IAS, Ali TI, Ibrahim OE (2011). Incidental occurrence and risk factors of brucellosis in teaching hospital. J. Adv. Med. Res. 1: 1 – 7.
Lapaque N, Forquet F, Chastellier CD, Mishal Z, Jolly G, Moreno E, Moriyon I, Heuser JE, Tao HH, Gorvel JP (2006). Characterization of Brucella abortus lipopolysaccharide macro domains as megarafts. Cellular Microbiol. 8(2): 197 – 206.
http://dx.doi.org/10.1111/j.1462-5822.2005.00609.x
PMid:16441431
Mohmand AQK, Humaira Z, Kiran TB (2012). Comparative studies of human brucellosis (Malta fever) in two provinces (Khyber PakhtunKhwa and Punjab) in patients suffering from febrile illness and PUO (Pyrexia of unknown origin). Isra Med. J. 4: 143 – 147.
Mrunalini N, Eddy RMS, Ramasastry P, Rao MR (2004). Sero–epidemiology of human brucellosis in Andhra Pradesh. Indian Vet. J. 81: 744 – 747.
Mukhtar F, Kokab F (2008). Brucella serology in abattoir workers. J. Ayub Med. Coll. Abbottabad. 20(3): 57 – 61.
PMid:19610518
Nielsen K, Duncan JR (1990). Epidemiology and surveillance of animal brucellosis. CRC. Press Boston. Pg. 131 – 151.
PMid:1695432
Omer MK, Assefaw T, Skjerve E, Tekleghiorghis T, Woldehiwet Z (2002). Prevalence of antibodies to Brucella spp. and risk factors related to high–risk occupational groups in Eritrea. Epidemiol. Infect. 129: 85 – 91.
http://dx.doi.org/10.1017/S0950268802007215
PMid:12211600 PMCid:PMC2869878
Queipo–ortuno MI, Pilar M, Ocon P, Manchado P, Colmenero JDD (1997). Rapid diagnosis of human brucellosis by peripheral–blood PCR assay. J. Clin. Microbiol. 2927 – 2930.
PMid:9350761 PMCid:PMC230089
Rabab A, Attas A, Khalifa MA, Al–Qurashi AR, Badawy M, Al–Gulay N (2000). Evaluation of PCR, culture and serology for the diagnosis of acute human Brucellosis. Ann. Saudi. Med. 20: 224 – 228.
Riaz R (2006). Seroprevalence of brucellosis in human and goats population of North Waziristan agency Pakistan. M.Sc Thesis, Hazara University, Mansehra.
Steven D (2012). Brucellosis. http://www.medicinenet.com/brucellosis.
Saeed KMI, Jamalludin A, Mohammad NS, Ahmad FG, Rana JA (2013). Concurrent brucellosis and Q fever infection: a case control study in Bamyan province, Afghanistan. Cen. A. J. global health. (http://cajgh.pitt.edu/ojs/index.php/cajgh/article/view/58/145)
Ohtsuki R, Kawamoto K, Kato Y, Shah MM, Ezaki T, Makino SI (2008). Rapid detection of Brucella spp. by the loop-mediated isothermal amplification method. J. App. Microbiol. 104: 1815 – 1823.
http://dx.doi.org/10.1111/j.1365-2672.2008.03732.x
PMid:18248366
Ruiz-Mesa JD, Sanchez-Gonzalez J, Reguera JM, Martin L, Lopez Palmero S, Colmenero JD (2005). Rose Bengal test: diagnostic yield and use for the rapid diagnosis of human brucellosis in emergency departments in endemic areas. Clin. Microbiol. Infec. 11: 221 – 225.
http://dx.doi.org/10.1111/j.1469-0691.2004.01063.x
PMid:15715720
Yohannes M, Tesfaye M, Hailu D, Tadele T, Mezene W (2012). Bovine brucellosis: serological survey in Guto-Gida district, East Wollega Zone, Ethiopia. Global Veterinaria. 8 (2): 139 – 143.



