Advances in Pharmaceutical and Ethnomedicines
Research Article
Advances in Pharmaceutical and Ethnomedicines 2 (2): 26 – 31Evaluation of Prescribing Trends in Ambulatory Cardiac Patients above 50 Years of Age in Lahore, Pakistan
Allah Bukhsh*, Sana Saif, Hafsa Imtiaz, Iram Arif, Aruba Muzaffar, Rabia Saleem
-
Institute of Pharmaceutical Sciences, University of Veterinary and Animal Sciences, Lahore, Pakistan
*Corresponding author:abukhsh@uvas.edu.pk
ARTICLE CITATION:
Bukhsh A, Saif S, Imtiaz H, Arif I, Muzaffar A, Saleem R (2014). Evaluation of prescribing trends in ambulatory cardiac patients above 50 years of age in Lahore, Pakistan. Adv. pharm. ethnomed.2 (2): 26 – 31.
Received: 2014–03–25, Revised: 2014–05–31, Accepted: 2014–06–01
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.ape/2014/2.2.26.31
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Cardiovascular problems are major cause of mortality in 85% of under developing countries. In Pakistan, elderly patients suffer with a number of cardiovascular problems like hypertension, myocardial infarction and ischemic heart disease; co–morbid conditions like diabetes, hypertension and dyslipidemias can increase the risk of cardiovascular problems. A concurrent, cross sectional study was designed to identify the incidence rate of cardiovascular problems, the associated co–morbid conditions and the pattern of drug prescribing among ambulatory cardiovascular patients (age ≥ 50 years). A total of 190 prescriptions were collected from various tertiary care hospitals of Lahore from September 2013 to November 2013 and were analyzed for prescribing practices. Our study concluded that most of the elderly patients were suffering with Myocardial infarction (35.7%) and Ischemic heart disease (35.7%). Hypertension (25.7%) and diabetes mellitus (13.6%) were the most frequent co–morbid conditions observed. The most commonly prescribed drugs in these patients were anti–platelets (85.2%), anti–hyperlipidemics (84.2%) and beta blockers (78.9%). Only 23% prescriptions were prescribed by generic name whereas dose, frequency and duration were mentioned in almost all prescriptions. Cardiovascular problems are approximately twice as frequent in patients with co–morbidities like diabetes and hypertension compared with patients without these co–morbidities. Therefore, in patients with co–existing co–morbidities strategies should be adopted for primary prevention and optimal control of these risk factors along with cardiovascular problems management.
INTRODUCTION
Prescribing for geriatric patients leads to unique challenges. Most of clinical trials are not performed on geriatric patients so the optimum doses selected for the drug might not be appropriate for the elderly patients (Cho S, 2011). Several drugs require special attention when to be used in the older patients because certain drugs may exhibit changes in the pharmacokinetics and pharmacodynamics depending on the age of the patient. Emphasis should be laid while selecting a dosage regimen for the elder patients. They have more volume of distribution as a result of increased proportion of fats in the body as compared to the skeletal muscles i.e. a physiological change with aging. Renal clearance is also reduced due to natural decline in renal function with age, regardless of renal disease (Rowe JW, 1976). Increased volume of distribution and decreased clearance lead to increased drug plasma concentrations in geriatrics.
Existing data of cardiac patients with ages above 50 years can offer valuable information for improving clinical practices. Quality of life of geriatric patients can be enhanced by raising the treatment standards in the health care system at all levels and auditing of these standards should be done (Curtis P, 1974). Rational prescribing is defined as the use of the minimum number of drugs to obtain the promising outcomes in the minimum time and at a reasonable cost (Gross F, 1981). Drug use in a health care facility not only indicates the approach and behavior of the prescriber, drug utilization trend but also indicate irrational practices like poly pharmacy and problems related to it (Hajjar ER, 2007). Cardiovascular diseases are usually chronic so there are higher chances of poly pharmacy. Cardiovascular diseases occur with other co–morbid conditions, e.g. Diabetes mellitus (Long AN, 2011). Pakistan is at number six in terms of number of diabetic patients up till 2009 but it is assumed to be at 4th rank up till 2020 and according to the report of health survey of Pakistan prevalence rate of diabetes was more in patients above 50 years of age (Wasay M, 2009). Most prevailing cardiovascular diseases in Pakistan are ischemia, myocardial infarction, stable angina, and hypertension. The current study was, therefore, aimed at identifying the patterns of drug utilization in cardiac patients above the age of 50 years having ischemia, myocardial infarction, stable angina, hypertension and many other prevailing cardiac diseases and to know if any co–morbid condition present in these patients in selected health facilities of Lahore, Pakistan.
MATERIALS AND METHODS
A concurrent and cross–sectional study was conducted from September 2013 to November 2013, by collecting the prescription data of ambulatory patients of age above 50 years suffering with cardiac problems from various tertiary care hospitals of Lahore, Pakistan. The patterns of drug use in ambulatory patients in various tertiary care hospitals and suffering from cardiovascular disorders were studied. A purpose based data collection Performa was used to collect the required information from the 190 ambulatory patients with cardiovascular disorders. The major patient parameters which were recorded include diagnosis, co–morbid conditions, and drug class prescribed. The drug parameters noted were; name of the drug, dose, method, frequency and duration of administration on patient prescription. The number of drugs that were prescribed to ambulatory patients and percentage of the drugs prescribed by their generic or brand name was also noted. Results are described by using descriptive statics in form of frequency distribution and percentages in bar charts and pie charts.
RESULTS
The dataset contain a total of 190 elderly cardiac patients of age above 50 years having cardiac problems alone or in combination with other co–morbidities. Out of which majority of the cardiovascular patients (35.7%) were suffering with myocardial infarction (MI), 35.7% with ischemic heart diseases (IHD) and 14.20% with hypertension. While other non frequent cardiovascular diseases were observed in less than 3% of the total patients as shown in Figure No.1
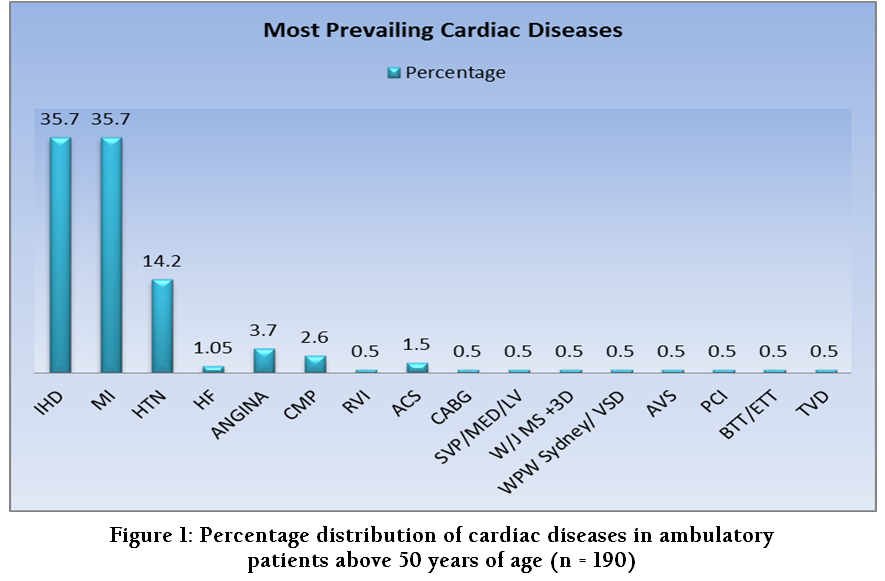
Figure 1: Percentage distribution of cardiac diseases in ambulatory patients above 50 years of age (n = 190)
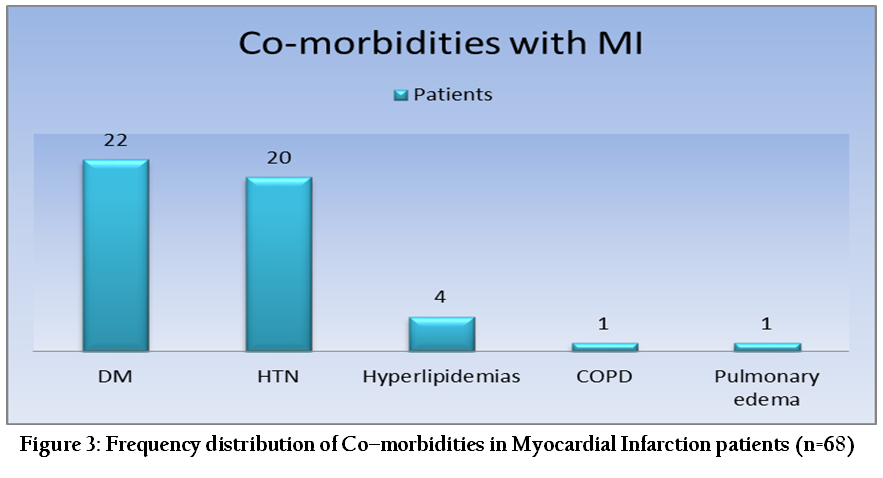
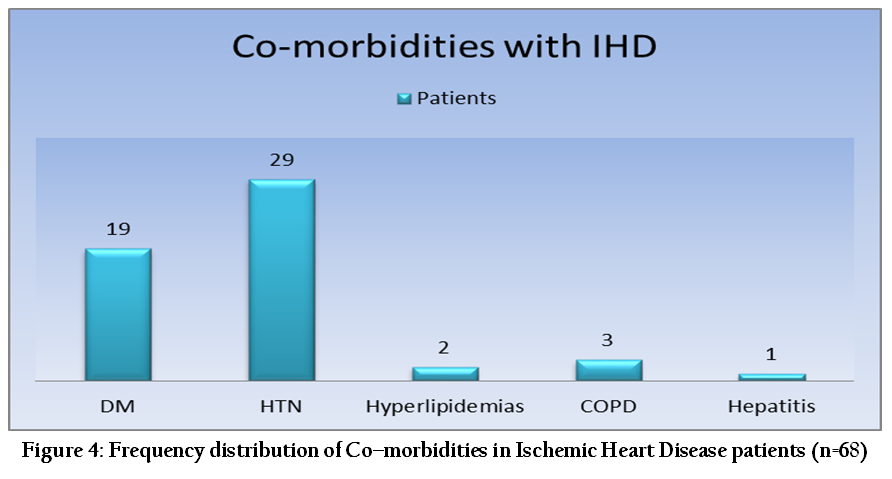
Co–morbidities are one of the leading causes of increasing complications and poor therapy outcomes in patients with cardiovascular problems. Out of 190 prescriptions which we evaluated in our study, 111 (58.4%) patients were suffering with various co–morbidities. Hypertension (47.7%) and diabetes militias (40.5%) were observed to be the most prevailing co–morbidities followed by hyperlipidemias (6.3%), COPD (3.6%), hepatitis (0.9%) and pulmonary edema (0.9%) as shown in figure 2. Out of 68 patients of MI, 48 patients (71%) were observed with co–morbidities out of which the major was diabetes mellitus observed in 22 patients, HTN in 20 patients, hyperlipidemias in 4 patients, COPD and pulmonary edema in 1 patient each, as shown in figure 3. Out of 68 patients who were observed to have IHD, 54 (79.5%) were with co–morbidities; with HTN in 29 patients, DM in 19 patients, COPD in 3, hyperlipidemias in 2 and hepatitis in 1 patient, while rest of the 14 patients of IHD did not have any co–morbidity as shown in figure 4.
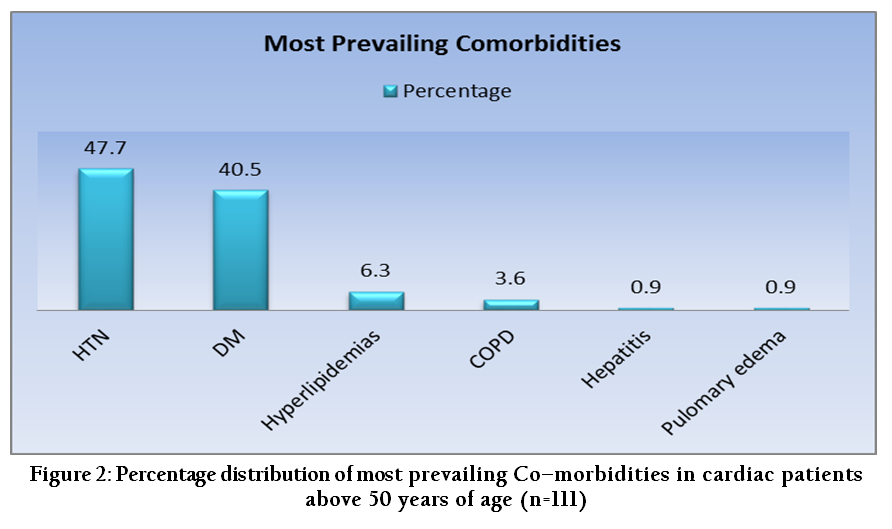
Figure 2: Percentage distribution of most prevailing Co–morbidities in cardiac patients above 50 years of age (n=111)
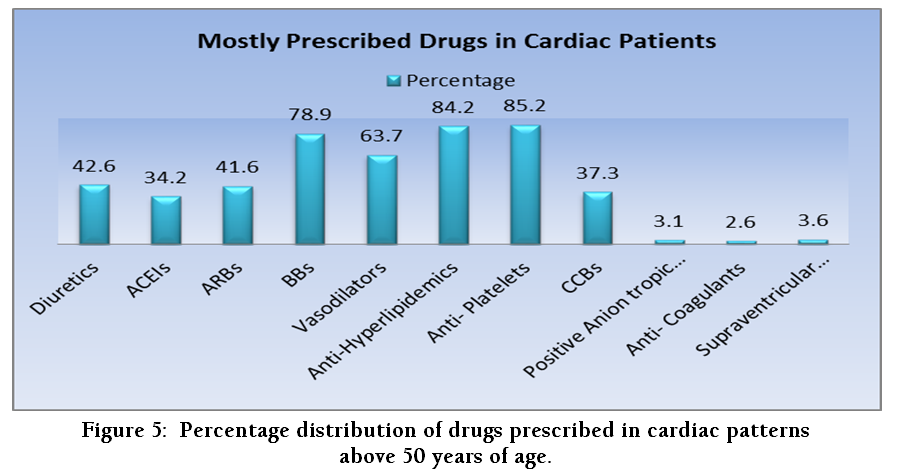
The drugs which were prescribed in cardiac patients were anti–platelets (85.2%), anti–hyperlipidemias (84.2%), beta blocker (78.94%), vasodilators (63.68%), anti–coagulants, diuretics (42.6%), ARBs (41.57%), CCBs (37.3%), ACEIs (34.2%), while infrequent drugs prescribed include supraventricular arrhythmic drugs (3.68%), positive anion tropic drugs (3.15%) and anti–coagulants (2.63%), as shown in figure 5.
MI patients were mostly prescribed with anti–hyperlipidemics (91.17%) followed by anti–platelets (86.29%) and diuretics (58.82%) as shown in figure no.6. Patients with HTN were prescribed with anti–platelets (74.07%), anti–hyperlipidemics (55.55%) and then diuretics (51.85%), whereas in IHD patients anti–platelets (91.17%), anti–hyperlipidemics (79.41%) followed by diuretics (54.41%) as shown in Figure No.6. At an average of 4 to 6 drugs are used in cardiovascular patients with various co–morbidities, based on diagnosis. Number of drug increases as the severity of the disease increases. Patients with severe IHD and MI were prescribed 6 to 7 drugs; some patients were being prescribed with 2 anti–platelets and 2 diuretics at same time leadings towards poly pharmacy.
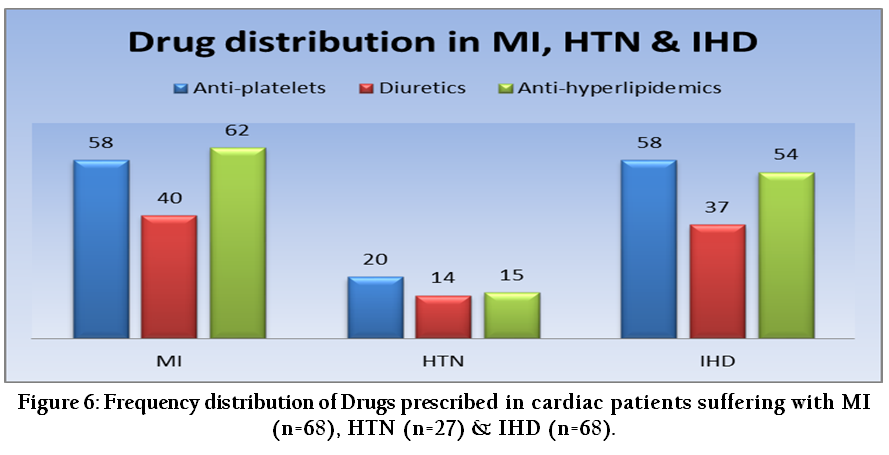
Figure 6: Frequency distribution of Drugs prescribed in cardiac patients suffering with MI (n=68), HTN (n=27) & IHD (n=68)
The drug parameters (name of the drug, dose, method, frequency and duration of administration) on prescription were observed quite satisfactory as shown in Table 1. Out of 190 prescriptions, number of the injectables and antibiotic prescribed were less than 3% which is a good practice.
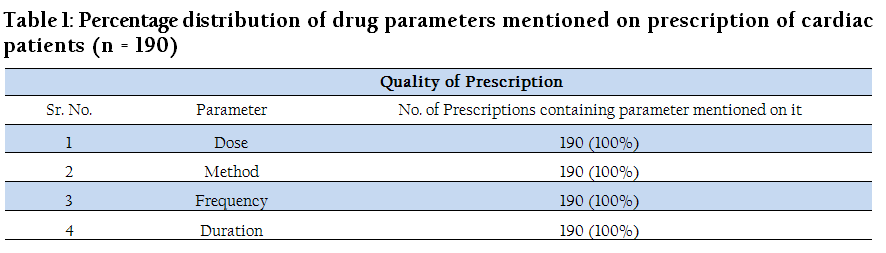
Table 1: Percentage distribution of drug parameters mentioned on prescription of cardiac patients (n = 190)
DISCUSSION
Prescribing in ambulatory elderly patients is a critical task; care must be taken in order to select an appropriate dosage regimen when prescribing for such patients (Siyal FJ, 2014). Cardiovascular disease includes numerous problems like myocardial infarction, ischemic heart disease, hypertension, etc, which are the leading causes of mortality in the world accounting for 29.3% of deaths per year. The prescribing in patients above 50 year of age with cardiac diseases needs to be carefully evaluated and the drug therapy should be specific relating to patient condition. As the chances of co–morbidity increases in older age, so prescribers should be more careful regarding drug–drug interaction, drug disease interaction and their side effects in older cardiac patients.
According to the WHO’s World Health Report, 58% of the deaths are caused by 15 common diseases and IHD is at the top of list with a percentage of 12.6 (WHO 1993). Our study findings corroborate WHO’s World Health Report as IHD is observed to be most frequently prevailing cardiac problem as shown in figure 1. But along with IHD, our study revels MI as another equally prevailing cardiac disease. The reason for IHD being on the top list in geriatric patient is impaired metabolism of cholesterol leading towards arteriosclerosis which reduces blood flow resulting into hypoxic conditions thus causing disease. Estimating total to HDL cholesterol ratio finds a significant relationship between dyslipidemia and development of coronary disease in the elderly. Similarly, MI for being frequently occurring cardiac problem in elderly is decline in maximal heart rate after exercise, diastolic filling of ventricle decreases and after load raises secondary to increased stiffness of ascending aorta because of which ability of ventricle to empty the chamber alters due to which diastolic pressure become higher and myocardial blood flow declines. Whereas our study concludes that non–frequent cardiac problems accounts in less number of patients (Figure 1).
Co morbidities complicate cardiovascular disease as they change biological response to therapy, disable the patients to get adhere to the recommendations given by health care professional resulting in alteration in the treatment outcomes (Wong CY, 2011). Most frequently occurring co–morbidities recorded in our study were Diabetes mellitus and hypertension followed by non–frequent diseases like hyperlipidemias, COPD, pulmonary edema and hepatitis as shown in figure 2. Diabetes is chronic increase in blood glucose level it could extensively cause myocardial damage causing heart failure and secondary stress because unfavorable long–term prognosis was improved by intensive insulin treatment which influences the chances of cardiac problems. Other possible reason for diabetes mellitus as a frequent co–morbid condition along with cardiovascular problems could be related to myocardial metabolism in which oxygen consumption increased from fatty acid instead of glucose oxidation. Thus, strike metabolic care should be monitored in such patients. DM and HTN are being frequent co–morbidities with MI & IHD (figure 3 & 4 ) such patients must have routine blood pressure checkups on every scheduled diabetes follow–up visit as diabetic patients with Bp > 130 mmHg systolic or > 80 mmHg diastolic are candidates for antihypertensive treatment and there treatment aim is to reduce Bp to < 130/80 mmHg (Arauz–Pacheco C, 2002). Co–morbidities of cardiovascular diseases like DM, HTN, hyperlipidemias, pulmonary edema and hepatitis are caused because of complex interrelationship and shared risk factors among them. Burden associated with it could be reduced by controlling risk factors and by improving disease management.
Mostly prescribed drugs by physicians to cardiac patients observed in our study were diuretics, ACE’S, anti–platelets, anti–hyperlipidemics, Beta blockers, CCB’s, ARB’s, anti–coagulants, positive anion tropic etc shown in figure 5. We have investigated 190 ambulatory cardiac patients out of which mostly were suffering with MI and IHD along with co–morbidities most likely DM and HTN and they were observed to be majorly prescribed with anti–platelets, anti–hyperlipidemics and diuretics (figure 6).
Poly pharmacy is one of major problem still unresolved in health care sector of developing and underdeveloped countries leading to number of adverse drug events in elderly patients. The Good Palliative–Geriatric Practice algorithm should be adopted to effectively reduce poly pharmacy and in improving quality of geriatric patient care (Garfinkel D, 2010). Poly pharmacy leads to increased risk of morbidity and mortality (Hajjar ER, 2007). During our study the average number of the drugs prescribed per prescription was 5.75 which comparatively very high as compared to WHO ideal value. As for as quality of prescription is concerned; dose, method of drug intake, duration of therapy, frequency of drug intake were mentioned on the 100 % prescriptions as shown in Table 1.

According to WHO core prescribing indicators generic prescribing should be observed in 100% prescriptions, but in our study we observed that generic prescribing was followed in only 23% of prescriptions as shown in Figure 7. There is a great variability in writing of prescription by the physicians and transcribing of that writing by the pharmacist because of non generic prescribing leading to misunderstanding of instructions for which universal medication schedules are being proposed to minimize the chances of adverse events (Wolf MS, 2011). In order to ensure quality prescribing there must be a presence of standard treatment guidelines at national and institutional level and mandatory continue education programs on Good prescribing Practices for health care providers. Cardiac rehabilitation programs should be conducted to prevent cardiovascular disorders involving education, counseling and motivating behavioral interventions to promote lifestyle modification (Goble AJ, 1999). Co morbidities like diabetes and hypertension can exacerbate cardiovascular problems, therefore, in patients with such co–existing conditions corrective measures should be adopted for primary prevention and optimal control of these risk factors. Such patients must be recommended for more aggressive treatment (i.e., reducing blood pressure to < 130/85 mm Hg) initially by dietary modifications, weight control and physical activities as it is remarkably an effective approach for primary prevention of co–morbidities while additionally in some patients, specific medications are required to achieve national treatment goals of diabetes and hypertension.
REFERENCES
Arauz-Pacheco C, Parrott MA, Raskin P (2002). The Treatment of hypertension in adult patients with diabetes. Diabetes Care. 25 (1): 134 - 147.
http://dx.doi.org/10.2337/diacare.25.1.134
PMid:11772914
Cho S, Lau SW, Tandon V, Kumi K, Pfuma E, Abernethy DR (2011). Geriatric drug evaluation: where are we now and where should we be in the future? Arch. Intl. Med. 171(10): 937 - 940.
http://dx.doi.org/10.1001/archinternmed.2011.152
PMid:21606098
Curtis P (1974). Medical audit in general practice. J. R. Coll. Gen. Pract. 24(146): 607 – 611.
PMid:4478845 PMCid:PMC2157429
Garfinkel D, Mangin D (2010). Feasibility study of a systematic approach for discontinuation of multiple medications in older adults. Arch. Intl. Med. 170 (18): 1648 - 1654.
http://dx.doi.org/10.1001/archinternmed.2010.355
PMid:20937924
Goble AJ, Worcester MUC (1999). Best practice guidelines for cardiac rehabilitation and secondary prevention. Heart Res. Cen. available at: http://www.health.vic.gov.au/nhpa/downloads/bestpracticecardiacrehab.pdf
Gross F (1981). Drug utilization - Theory and practice the present situation in the Federal Republic of Germany. Eur. J. Clin. Pharmacol. 19 (6): 387 - 394.
http://dx.doi.org/10.1007/BF00548580
PMid:7250171
Hajjar ER, Cafiero AC, Hanlon JT (2007). Poly pharmacy in elderly patients. Am. J. Geriatr. Pharmacother. 5(4): 345 - 351.
http://dx.doi.org/10.1016/j.amjopharm.2007.12.002
PMid:18179993
Long AN, Dagogo-Jack S (2011). The Comorbidities of diabetes and hypertension mechanisms and approach to target organ protection. J. Clin. Hypertens. 13(4): 244 – 251.
http://dx.doi.org/10.1111/j.1751-7176.2011.00434.x
PMid:21466619 PMCid:PMC3746062
Rowe JW, Andres R, Tobin JD, Norris AH, Shock NW (1976). The effect of age on creatinine clearance in men: a cross-sectional and longitudinal study. J. Gerontol. 31 (2): 155 - 163.
http://dx.doi.org/10.1093/geronj/31.2.155
PMid:1249404
Siyal FJ, Dayo A, Sial JA, Ghoto MA, Malik A, Memon N, Rajput J, Shaikh RA (2014). Prescription trend of challenging problems in cardiac patients of Larkana Pakistan. Int. J. Pharm. Sci. Rev. Res. 24(1): 263 -267.
Wasay M, Jabbar A (2009). Fight against chronic diseases (high blood pressure, stroke, diabetes and cancer) in Pakistan; cost-effective interventions. J. Pak. Med. Assoc.59(4): 196 - 197.
PMid:19402275
WHO (1993). How to Investigate Drug use in health facilities. Available at : http://apps.who.int/medicinedocs/pdf/s2289e/s2289e.pdf
Wolf MS, Curtis LM, Waite K, Bailey SC, Hedlund LA, Davis TC, Shrank WH, Parker RM, Wood JJA (2011). Helping patients simplify and safely use complex prescription regimens. Arch. Intl. Med. 171(4): 300 – 305.
http://dx.doi.org/10.1001/archinternmed.2011.39
PMid:21357804 PMCid:PMC3968427
Wong CY, Chaudhry SI, Desai MM, Krumholz HM (2011). Trends in comorbidity, disability, and polypharmacy in heart failure. Am. J. Med. 124 (2): 136 – 1.
http://dx.doi.org/10.1016/j.amjmed.2010.08.017
PMid:21295193 PMCid:PMC3237399



