Advances in Pharmaceutical and Ethnomedicines
Research Article
Advances in Pharmaceutical and Ethnomedicines 2 (2): 21 – 25Prescription Analysis of Ambulatory Patients of Diabetes Mellitus in Lahore Pakistan
Allah Bukhsh*, Iqra liaqat, Sehrish Javaid, Mussarat Bashir, Busma Khan, Humaira Yaseen, Momina Nadeem
-
Institute of Pharmaceutical Sciences, University of Veterinary and Animal Sciences, Lahore Pakistan
*Corresponding author:abukhsh@uvas.edu.pk
ARTICLE CITATION:
Bukhsh A, liaqat I, Javaid S, Bashir M, Khan B, Yaseen H, Nadeem M (2014). Prescription analysis of ambulatory patients of diabetes mellitus at Lahore Pakistan. Adv. Pharm. Ethnomed. 2 (2): 21 – 25.
Received: 2014–03–16, Revised: 2014–05–22, Accepted: 2014–05–23
The electronic version of this article is the complete one and can be found online at
(
http://dx.doi.org/10.14737/journal.ape/2014/2.2.21.25
)
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
ABSTRACT
Diabetes mellitus is one of the leading causes of mortality and morbidity worldwide. Its incidence rate appears to be increasing in the last few decades. In this study prescribing pattern of medications in 100 ambulatory patients of diabetes mellitus was observed from September 2013 to December 2013 in Lahore. It was revealed from our study that diabetes mellitus was more prevalent in patients of age above 30 years (96%) & incidence rate was higher in females (61%) as compared to males. 72% prescriptions were legible, dose was missing in 26% of the prescription, frequency in 38% and strength of medicines in 27%. Either of insulin or oral hypoglycemic agent was prescribed in 46% of the prescriptions as monotherapy. Biguanides were the most prescribed oral hypoglycemic agents as monotherapy (33%) & insulin alone in 13% patients. Combination of antidiabetic agents was observed in 54% prescriptions and frequently prescribed combination was of Sulfonylureas with Biguanides (41%).
INTRODUCTION
Diabetes mellitus is a metabolic disorder characterized by abnormal carbohydrate metabolism that leads to the hyperglycemia. It is related with a comparative or absolute deficiency of insulin secretion or resistance to the action of insulin (Ogedengbe OS, 2009). It has been increasing in prevalence since last decades and currently affects more than 170 million people worldwide (Patel H et.al, 2006). In Pakistan its prevalence is high ranging from 7.6 to 11% (Hakeem R, Fawwad A 2010). Type 1 diabetes or juvenile–onset diabetes is categorized by an absolute deficiency of insulin due to autoimmune–mediated destruction of the pancreatic beta cells that are responsible for the production of insulin (Cuthbertson D, 2008). Type 2 Diabetes or maturity–onset diabetes is the most prevalent type of diabetes (~90%) and is associated with high morbidity and mortality (Lusignan S et al., 2005) and is characterized by fluctuating degrees of resistance to the action of insulin with comparative insulin deficiency (Sperl–Hillen J 2012). Type 3 Diabetes or Brain diabetes having known reasons that brain instantaneously needs glucose. It can occur due to infections, sepsis hormonal changes, drugs and stress. It is also the cause of Alzheimer’s disease (Steen E et al., 2005). In Type 4 diabetes or gestational diabetes, body is under metabolic and physiological stress because the fetus consumption of glucose increases. In the patients with Type 4 diabetes, indication for insulin therapy is ineffective but exercise and nutritional therapy affects the prandial and fasting blood glucose levels (Mwanri W A et al., 2014).
Diabetes mellitus is diagnosed by a blood sugar tests either by fasting test (no food or fluid taken except water for eight hours) or a random test taken anytime during the day (2hr after a meal), or by Oral Glucose Tolerance Test or by HbA1C( every 2–3 months) (Sperl–Hillen J 2012). The criteria for diagnosis of diabetes mellitus is based on the values of fasting blood glucose test, random blood glucose test and HbA1C, which are ≤ 126mg/dl, ≤ 200mg/dl and ≤6.5 % respectively for normal healthy individuals (American Diabetes Association. Diabetes care, 2013).
Diabetes mellitus is managed by pharmacological and non–pharmacological ways. Pharmacological treatment includes oral hypoglycemic agents and subcutaneous agents (Alwan AAS, 1994). Oral hypoglycemic agents include insulin sensitizers (Biguanides, Thiazolidinediones), secretagogues (Sulfonylureas, Glinides), alpha glucosidaseinhibitors, DPP–IV inhibitors (Dipeptidyl peptidase–IV inhibitors), and others (Rapid release bromocriptine). Subcutaneous agents are GLP–1 analogue (Exenatide, Liraglutide, Extended release exenatide), Incretin (Pramlintide), Insulin that includes Rapid–Acting (Aspart, Lispro, Glulisine), Short–Acting (Regular) Intermediate (Neutral Protamine Hagedorn), Long–Acting (glargine, detemir), Premixed (Humalog mix 50/50 and 75/25) and (NovoLog mix 70/30) (Lub R et al., 2006).
Non–Pharmacological management includes dietary management, physical activity and stress management (Alwan AAS, 1994). Dietary Management includes chunks of food including cereals, mixed coarse grains, whole pulses, salads, red rice, fruits and vegetables (low GI), brown bread ,dietary fibers (oats, pulses), proteins and Saturated fat (ghee, butter). Sugar, honey, jaggery, sweets, white rice, white bread (high GI), hydrogenated fat must be avoided (Diabetes Management in General Practice, Guidelines for type 2 diabetes, 2012). Dietary cholesterol intake should be <300mg/day. Physical Activities include regular exercise which is essential; brisk walk 30min/day & 150min/week. As the exercise leading to the benefits which are ; improvement in insulin sensitivity, weight management, improvement of lipid profile, improvement of the function of CVS, increase in bone density, improvement of the quality of life, mental and physical wellness (Alwan AAS, 1994). Stress management includes behavioral modification (Positive thinking), meditation, appropriate support and counseling; improve skills (reading, writing, poetry) (Phan H et al., 2012). Study of prescribing practice, health facility or aggregate data indicators may indicate that there is over or under–consumption of medicines and these qualitative studies may indicate the reason that why certain health staff and patients behave the way they do. However, such studies do not give details about the exact nature of irrational use of medicines (Subhasish S et al., 2010).
The purpose of study was to evaluate the prescription patterns of anti–diabetics using WHO prescribing indicators (Khan AA et al., 2013; Angamo MT et al., 2011; Mahallie AAE , 2012). Prescriptions were analyzed after grouping the anti–diabetic medications by their respective therapeutic classes: sensitizers, secretogogues, alpha glucosidase inhibitors, DPPIV inhibitors, GLP1 analogue, Incretin and Insulin. Study parameters for ambulatory diabetic patients included WHO core and complementary indicators; which were, average number of anti–diabetic drugs per prescription, percentage of drugs prescribed by generic name (Duerden M et al., 2011), percentage of prescriptions with an insulin prescribed, percentage of prescriptions with dose mentioned, percentage of prescriptions with legible handwriting, percentage of prescriptions with dose frequency and strength of drug mentioned in it. (Alwan AAS, 1994; Khan AA et al., 2013; Angamo MT et al., 2011). The most common preference as drug of choice in a community; either oral hypoglycemic agents or insulin was also evaluated. Prescribing errors have the potential to cause serious side effects in diabetic patients. Poor hand writing, improper communication and the use of inappropriate abbreviations are also amongst the major prescribing errors (Khan AA et al., 2013).
MATERIAL AND METHOD
In this descriptive, qualitative, cross sectional study, data were collected from prescriptions of ambulatory diabetic patients by general practitioner's (GP’s) practicing in different clinics of Lahore, from September 2013 to December 2013. For this purpose 100 prescriptions were collected from various areas of Lahore. A questionnaire was designed by using WHO core and complementary indicators. The Prescribing indicators of WHO used for this study included, average number of drugs per prescription, percentage of drugs prescribed with generic names, and percentage of encounters with legible hand writing (Khan AA et al.,2013; Angamo MT et al., 2011). All the outpatients with diabetes mellitus either with type 1 or type 2 were included in the study except inpatient, pregnant and lactating women. The independent variables in this study were age and gender of the patient. The dependent variables were average number of anti–diabetics; percentage of drugs prescribed with generic name, legible handwriting, prescriptions containing insulin and mentioned dose, frequency and strength of drug (Carey N et al., 2008; Angamo MT et al., 2011). We grouped prescription data of anti–diabetic medications by therapeutic class which included oral anti–diabetic drugs and injectable anti–diabetic drugs. Data obtained were analyzed by using SPSS version 16.0 statistical software programs. Results were analyzed descriptively in the form of percentages and presented in tabulation form according to the tool types (Alexander CG et al., 2008).
RESULTS
The age of majority of patients in study was observed to be above 30 years (n=96) as shown in Figure 1.
According to clinical characteristics and demographics, females were observed more prone to diabetes mellitus in our study (n=61) as compared to male patients as shown in Figure 2.
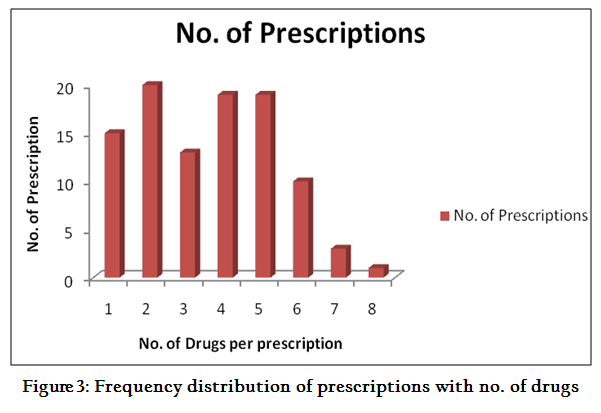
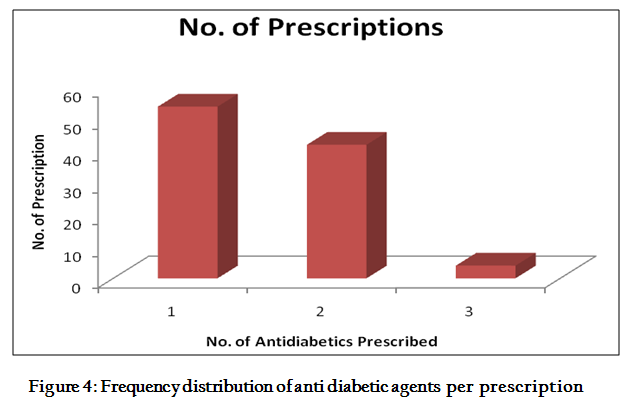
Average number of drugs (anti diabetic and non anti diabetic) prescribed per prescription was 3.5 whereas antidiabetic drugs per prescription were 1.5 as shown in Figure 4. 48% prescriptions contained 3 or less drugs per prescription, 38% prescriptions contained 4 or 5 drugs per prescription and 14 % prescriptions contained more than 5 drugs per prescription as shown in Figure 3.
Generic name of the medicines was mentioned in only 16% prescriptions (11% of antidiabetics and 5% other drugs) as shown in Figure 5 and in 28% prescriptions handwriting was illegible. Dose was missing in 26% of the prescription, frequency in 38% and strength of medicines in 27% of prescriptions. Either insulin or oral hypoglycemic agent was prescribed in 54% of the prescriptions. Biguanides were the most prescribed oral hypoglycemics as monotherapy (33%) as shown in Table. No. 2 & insulin alone in 13%, out of which 10% prescriptions contained premixed insulin, 2% short acting insulin and 1% intermediate acting insulin. Combination of antidiabetic agents was observed in 46% prescriptions. Combination of oral anti diabetic agents was observed in 43% prescriptions. Frequently prescribed combination was of Sulfonylureas with Biguanides (41%) and combination of three oral anti–diabetic drugs (biguanides + sulphonylureas + thaizolidinediones) was observed in 2 % prescriptions. Combination of various types of insulin with oral anti diabetic agents was observed in 3% of prescriptions. 1% prescriptions contained combination of premix insulin and diasaccahridase inhibitor, 1% prescription with combination of premix insulin and two oral anti–diabetics (biguanides + sulphonylureas). Combination of oral anti–diabetic drugs (biguanides) and pre mixed insulin was least frequently prescribed (1 %) as shown in Table 1 and Figure 6.
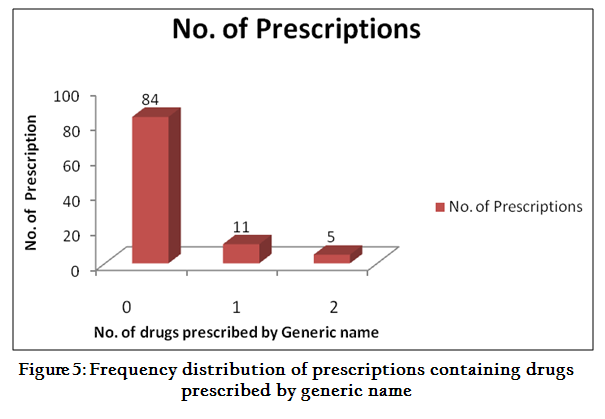
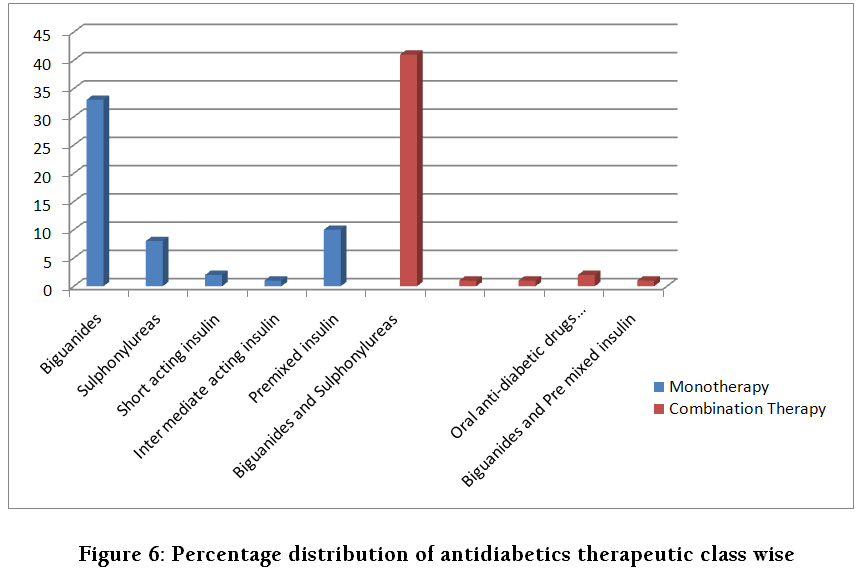
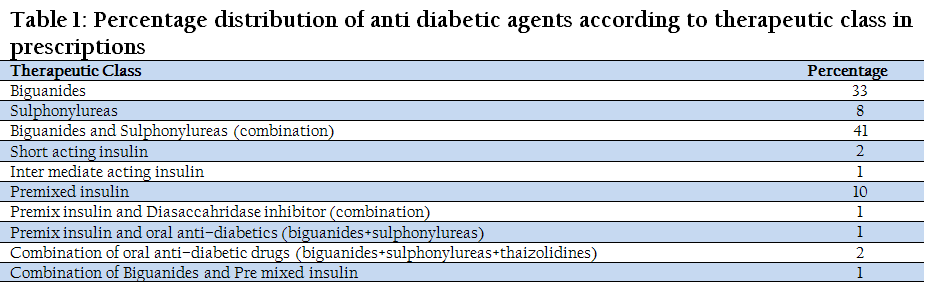
Table 1: Percentage distribution of anti diabetic agents according to therapeutic class in prescriptions
DISCUSSION
Based on the prescription analysis data, 100 prescriptions of diabetic patients selected randomly from various areas of Lahore were analyzed. In this study, the high prevalence (96%) of diabetes was observed in patients above 30 years as shown in Figure 1. A study conducted at U.S. and UK showed the similar result (Phan H et.al,2012) In our study the rate of occurrence of diabetes in females was greater (61%) than that of males (39%) as shown in Figure 2. WHO core and complementary indicators were used in this study to analyze the prescribing trends in ambulatory diabetic patients. According to WHO, average number of drugs per prescription should be 1.6 – 1.8 (Desalegn AA 2013), in our study average number of drugs per prescription was 3.5, which is almost double to the WHO standard (Figure 3). Average number of anti diabetic agents was observed to be 1.5 (Figure 4), same trend was observed in similar studies conducted at Karachi, Pakistan and Southwest Ethiopia (Khan AA et al., 2013; Angamo MT et al., 2011). It was observed that only 16 % drugs were prescribed by generic name (Figure 5) which is very low as compared to WHO standard which is 100% (Desalegn AA 2013). Mono therapy was observed in 46% of prescriptions and combination therapy in 54% (Figure 6). Biguanides were the most frequently prescribed agents (33%) as monotherapy (as represented by A in Figure 6). A similar trend of biguanides prescribing was also observed in a study performed in UK (Fillion KB et al., 2009). A similar study conducted in Italy and Manitoba in which the prescribing percentage of biguanides was also high (Mazzagliaa G et al., 2008; Ludwig SM et al., 2006). Mostly prescribed insulin as mono therapy (10%) was premixed insulin followed by short acting insulin (2%) and intermediate acting insulin (1%) as represented in Figure 6.
Combination of biguanides and sulphonylureas was mostly prescribed (41%) as shown in Figure 6. A study conducted in US in 2008, showed similar higher proportion of same combination of oral anti diabetic agents (Alexander CG et al., 2008). Combination of three oral anti diabetic drugs (biguanides + sulphonylureas + thaizolidindiones) was observed in 2% prescriptions (Figure 6). A combination of oral anti–diabetic drugs (biguanides) and pre mixed insulin was prescribed on 1% prescriptions (Figure 6). Another similar study conducted at Italy in which the same results were obtained (Mazzagliaa G et al., 2008). Combination of premixed insulin and diasaccahridase inhibitors was in 1% (Figure 6.) and combination of premix insulin and oral anti–diabetic drugs (biguanides+ sulphonylureas) in 1% (Figure 6).
Biguanides were the most prescribed oral hypoglycemic agents alone and in combination with sulfonylureas. Poor prescribing practices were observed as for as generic prescribing and average number of drugs were concerned. This study appears to suggest that prescribing practices should be in line with the recent scientific evidences. There is a need to develop Diabetes mellitus management guidelines and Continual Education (CE) programs on Good Prescribing Practices for family physicians in order to meet the WHO standards for prescribing practices.
ACKNOWLEDGEMENT
The authors humbly pay their profound gratitude to Vice Chancellor Prof. Dr. Talat Naseer Pasha, University of Veterinary and Animal Sciences Lahore, Pakistan and head of Pharmacy Department Dr. Farzana Chowdhary, Institute of Pharmaceutical Sciences, for their kind support and special attention throughout this study project.
REFERENCES
Alexander CG, Sehgal NL, Moloney RM, Stafford RS (2008). National Trends in Treatment of Type 2 Diabetes Mellitus. 1994–2007. JAMA. 168(19): 2088–2094
Alwan AAS (1994). Management of Diabetes Mellitus Standards 0f Care and Clinical Practice Guidelines. In WHO–EM/DIN6/E/G. Available at: http://applications.emro.who.int/dsaf/dsa509.pdf ((May 2014, date last accessed)
Angamo MT, Wabe NT, Raju NJ (2011). Assessment of Patterns of Drug use by using World Health Organization's Prescribing, Patient Care and Health facility indicators in Selected Health Facilities in Southwest Ethiopia. JAPS. 1(07): 62–66
Carey N, Stenner K, Courtenay M (2008). Prescription writing for patients with diabetes: compliance with good practice. Nurse Prescribing. 7(10):1–15
Cuthbertson D (2008). In: Synopsis of Causation Diabetes Mellitus. Available at: http://www.veterans-uk.info/publications/diabetes_mellitus.pdf (May 2014, date last accessed)
Desalegn AA (2013). Assessment of drug use pattern using WHO prescribing indicators at Hawassa University teaching and referral hospital, south Ethiopia: a cross–sectional study. BMC Health Serv Res. 13:1–6
http://dx.doi.org/10.1186/1472-6963-13-170
PMid:23647871 PMCid:PMC3651314
Diabetes Management in General Practice, Guidelines for type 2 diabetes (2012). Diabetes Australia. Available at: http://www.diabetesaustralia.com.au/Documents/DA/What's%20New/12.10.02%20Diabetes%20Management%20in%20General%20Practice.pdf (May 2014, date last accessed)
Duerden M, Millson D, Avery A, Smart S (2011). The quality of GP prescribing. The King's Fund. 1–118
Filion KB, Joseph L, Boivin FJ¸ Suissa S, Brophy JM (2009). Trends in the prescription of anti diabetic medications in the United Kingdom: a population–based analysis. Pharmacoepidemiol Drug Saf. 18: 973–976.
http://dx.doi.org/10.1002/pds.1802
PMid:19621344
Hakeem R, Fawwad A (2010). Diabetes in Pakistan: Epidemiology, Determinants and Kennedy DL, Piper JM, Baum DC (1988). Trends in Use of Oral Hypoglycemic Agents 1964–1986. Diabetes Care. 11(7):558–562
Khan AA, Marvi, Iqbal J,Nadeem M (2013). Prescribing Practices of General Practitioners of Public Hospitals of Pakistan. WJPR. 2(2):285–296.
Lub R, Denig P, Berg BP, Hoogenberg K, Berg WTL, (2006). The impact of new insights and revised practice guidelines on prescribing drugs in the treatment of Type 2 diabetes mellitus. Br. J. Clin. Pharmacol. 62(6): 660–665.
http://dx.doi.org/10.1111/j.1365-2125.2006.02711.x
PMid:16796700 PMCid:PMC1885194
Ludwig SM, Griffith JE, McQuillen KI, Anderson WA, Kvern BL (2006). Manitoba Diabetes Care Project: Examining Trends in Diabetes Therapy Prescribing Patterns in Manitoba. Can. J. Diabetes. 30(3):248–255.
http://dx.doi.org/10.2337/diacare.29.02.06.dc05-1771
Lusignan DS, Sismanidis C, Carey I M, DeWilde S, Richards N and Cook DG (2005). Trends in the prevalence and management of diagnosed type 2 diabetes 1994–2001 in England and Wales. BMC FAM PRACT. 6(13):1–8.
Mahalli AA (2012). WHO/INRUD drug prescribing indicators at primary health care centers in Eastern province, Saudi Arabia, 1College of Applied Medical Sciences, University of Dammam, Dammam, Saudi Arabia; and Department of Health Administration and Behavioural Sciences. East Mediterr Health J. 18(11):1091–1096
PMid:23301369
Mazzagliaa G, Yurginb N, Boyeb SK, Trifiro G, Cottrelle S, Allene E, Filippi A, Medeaa G, Cricelli C (2008). Prevalence and Antihyperglycemic prescribing trends for patients with type 2 diabetes in Italy: A 4–year retrospective study from national primary care data. PHARMCOL RES. 57:358–363.
http://dx.doi.org/10.1016/j.phrs.2008.03.009
PMid:18455425
Mwanri WA, Kinabo J, Ramaiya K, Feskens MJE (2014). Prevalence of gestational diabetes mellitus in urban and rural Tanzania. DIABETES RES CLIN PR. 103:71 – 78.
http://dx.doi.org/10.1016/j.diabres.2013.11.021
PMid:24367971
Ogedengbe OS (2009). Synopsis of diabetes mellitus. POSTGRAD MED J. 11 (1): 101–107
Patel H, Srishanmuganathan J, Car J, Majeed A (2006). Trends in the prescription and cost of diabetic medications and monitoring equipment in England 1991–2004. J Public Health. 29 (1):48–52
http://dx.doi.org/10.1093/pubmed/fdl076
PMid:17124257
Phan H, Porter K, Sill B, Nahata CM (2012). Prescribing Trends for the Outpatient Treatment of Adolescents and Young Adults with Type 2 Diabetes Mellitus. J Manag Care Pharm . 18(8): 607–614
PMid:23127148
Sperl–Hillen J (2012). Institute for Clinical Systems Improvement. Diagnosis and Management of Type 2 Diabetes Mellitus in Adults. In Health Care Guideline, Institute for Clinical Systems Improvement. 15: 1–141
Steen E, Terry MB, Enrique JE, Cannon LJ, Cannon, Neely RT, Tavares R, XJ, Wands RJ, Monte MS (2005). Impaired insulin and insulin–like growth factor expression and signaling mechanisms in Alzheimer's disease – is this type 3 diabetes. J Alzheimers Dis. 7: 63–80.
PMid:15750215
Subhasish S, Kaushik KD, Sabita S, Debasish S (2010). Prescription Analysis in Diabetes Mellitus. Int. J Pharm. Bio. Sci. 1: 1–8.



