Journal of Animal Health and Production
Case Report

Dystocia Due to Foetal Anasarca and Foetal Ascites with Concurrent Live Foetus in a Multiparous Malabari Doe
Sherin B. Sarangom1*, Varsha Mary Mathai2, Hiron M. Harshan3, C. P. Prasad4, K. Muraleedharan1, Seeja Sundaran1
1Veterinary Surgeon, District Veterinary Centre, Kannur, Kerala, India; 2Emergency Veterinary Services, Veterinary Polyclinic, Taliparamba, Kannur, Kerala, India; 3Assistant Professor, DARG&O, CV&AS, Mannuthy, Thrissur, Kerala, India; 4 Chief Veterinary Officer, District Veterinary Centre, Kannur, Kerala, India.
Abstract | A three-year-old full-term Malabari doe in her third parity was referred for dystocia due to abnormal large and disproportionate foetus, presented with oedematous limbs and scrotum, trapped and hanging from the birth canal in a lumbo-sacral position. Based on clinical and per-vaginal examination findings, the condition was diagnosed as dystocia due to concurrent foetal anasarca and ascites. Successful management of dystocia due to foetal anasarca and foetal ascites by foetal abdomen puncture and foetotomy per vaginum in a Malabari doe with concurrent live foetus delivered per vaginum is hereby reported.
Keywords | Foetal anasarca, Foetal ascites, Dystocia, Malabari doe, Foetotomy
Received | June 08, 2020; Accepted | June 14, 2020; Published | September 15, 2020
*Correspondence | Sherin B. Sarangom, Veterinary Surgeon, District Veterinary Centre, Kannur, Kerala, India; Email: sbs04vet@gmail.com
Citation | Sarangom SB, Mathai VM, Harshan HM, Prasad CP, Muraleedharan K, Sundaran S (2020). Dystocia due to foetal anasarca and foetal ascites with concurrent live foetus in a multiparous malabari doe. J. Anim. Health Prod. 8(4): 168-170.
DOI | http://dx.doi.org/10.17582/journal.jahp/2020/8.4.168.170
ISSN | 2308-2801
Copyright © 2020 Sarangom et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Dystocia due to foetal anomalies and monsters are more frequent in cattle than in sheep and goats (Hanie, 2006). Although infrequent, several foetal anomalies and monsters have been documented as causes of dystocia in small ruminants especially goats (Sharun and Erdogan, 2019). These may arise from adverse factors affecting the early developmental stages of foetus, mostly genetic mutations, but also include prenatal viral infections, physical factors, intrauterine exposure to poisons and deficiency of vitamins (Jones et al., 1997). Foetal anasarca signifies general dropsy of subcutaneous tissue, occurs either alone or accompanied by other anomalies and is less commonly reported in kids. Though the condition with ascites is most commonly reported in cattle (Roberts, 1971), it is sporadically reported in goats too including Malabari goats (Philip et al., 2012), the native breed of goats in Kerala (Verma et al., 2009). However, reports of concurrent presentation of foetal anasarca and ascites along with a normal live twin kid in Malabari goat could not be traced. The present paper describes successful management of dystocia due to foetal anasarca and foetal ascites by foetal abdomen puncture and foetotomy in a Malabari doe with concurrent live foetus delivered per vaginum.
Case Details
A three-year-old full-term Malabari doe in her third parity was referred to the outpatient unit of District Veterinary Centre, Kannur, Kerala, India for dystocia due to an abnormally large foetus. The chorioallantois had ruptured three hours back and the animal was straining. The physiological parameters of the doe were found to be normal. On per vaginal examination, after washing of perineum with 1 in 10000 potassium permanganate lotion, the vulva appeared swollen and oedematous with slightly congested vaginal mucous membrane. Oedematous limbs and scrotum of a foetus in posterior longitudinal presentation and lumbo-sacral position were found trapped and hanging from the birth canal (Figure 1A). Per-vaginal examination of
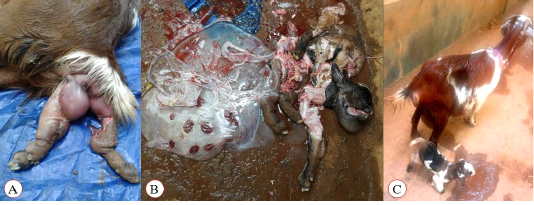
Figure 1: Malabari doe referred for dystocia due to abnormally large foetus. (A): oedematous limbs and scrotum of the foetus in dosrso-sacral position trapped at the birth canal; (B): the dead anasarcous foetus retrieved
by abdomen puncture and foetotomy along with the foetal membranes; and (C): the doe and the kid on the next day after obsterical procedure.
foetus after repulsion revealed that it was large sized and disproportionate with a severely distended abdomen that fluctuated on pressure indicating the presence of copious fluid. The vital reflexes of the foetus were absent. Based on the clinical and per-vaginal examination findings, the condition was tentatively diagnosed as dystocia due to concurrent foetal anasarca and ascites. Attempts to relieve the dystocia by gentle traction after sufficient lubrication were unsuccessful due to the distended abdomen and abnormally large size of the foetus leading to foeto-maternal disproportion. Since the foetus was confirmed as dead, a partial foetotomy of the foetus was resorted to with an aim to reduce the size of the foetus. The doe was administered epidural anaesthesia with 3 mL of 2% of lignocaine hydrochloride (Xylocaine 2%, AstraZeneca Pharma India Limited, Dundigal post, India) into the sacro-coccygeal epidural space. After lubrication with carboxy methyl cellulose, a gloved hand was inserted into the uterus and the foetal abdomen was punctured with an obstetrical hook followed by partial foetotomy using a Syme’s abscess knife to reduce the size of the foetus and retrieve the male foetus per-vaginum. Approximately six litres of ascitic fluid was drained out and the foetal parts including the eviscerated abdominal viscera were removed with gentle traction. On examination of the dead foetus, generalized oedema was observed with an enlarged and disproportionate head, swollen scrotal sac, puffed-up chin, rounded short neck and stumpy limbs, fairly developed hair coat and very thin skin. The foetal membranes along with the entrapped fluids were also removed (Figure 1B). Thereafter, one live, healthy female kid was also delivered per vaginum (Figure 1C). The doe was administered with Dextrose Normal Saline (Infutec Healthcare Ltd., Indore, India) at the rate of 10 ml/Kg body weight intravenously followed by ceftriaxone (Intacef, Intas pharmaceuticals, Ahmadabad, India) at the rate of 10 mg/Kg body weight, meloxicam (Melonex, Intas pharmaceuticals, Ahmadabad, India) at the rate of 0.2 mg/Kg body weight, oxytocin (Taj Pharmaceuticals Ltd., Mumbai, India) 5 IU (total dose) and tetanus toxoid (Serum Institute of India Pvt. Ltd., Pune, India) intramuscularly along with intrauterine administration of uterine cleanser. Antibiotic and antiinflammatory agents were continued for four more days and the animal had an uneventful recovery.
Discussion
Dystocia in large ruminants are common and are often due to foetal maldisposition and foetal anomalies (Hanie, 2006). In small ruminants, the incidence of dystocia has been reported to be less than 5% (Bhattacharyya et al., 2015). Foetal anasarca is frequent in bovines, but is rare in small ruminants (Purohit, 2006). The definite cause of foetal anasarca is unknown and may be associated with achondroplasia or lymphoid tissue agenesis possibly due to existence of an autosomal recessive gene defect (Long, 1996; Monteagudo et al., 2002). Foetal anasarca usually develops in a single foetus alone. Rarely, foetal anasarca occurs in association with other foetal anomalies or monsters too (Jayachandra et al., 2013) and in the present case it was diagnosed along with foetal ascites. The foetal ascites may be the result of obstruction of the lymphatics that prevents the disposal of peritoneal fluid (Roberts, 1971). In the present case, a concurrent live twin foetus was also delivered per vaginum and the presence of this normal foetus would have helped in maintaining the pregnancy in spite of foetal anomalies as observed by Prabaharan et al. (2016). The affected foetus was carried to full term and there was lack of progress in second stage of labor due to the foeto-maternal disproportion arising as a result of increased foetal size caused by accumulation of excess fluid in subcutaneous tissue and abdomen. Per-vaginal puncture of foetal abdomen facilitated the removal of ascitic fluid and foetotomy enabled the successful retrieval of the anomalous foetus to relieve dystocia which may otherwise have resorted to caesarean section (Winter, 1999). In small ruminants, such an association of foetal anasarca and foetal ascites along with a concurrent live twin foetus was previously reported in an indigenous kid by Prabaharan et al. (2016) and the present case is a rare report in a Malabari doe, a native breed of Kerala. Although the ultrasonographic antenatal monitoring for gestational foetal anomalies is warranted to avoid potential peripartum complications (Suguna et al., 2008), the presence of concurrent live foetus remains a concern if termination has to be executed. The successful management of dystocia due to both foetal anasarca and ascites by foetal abdomen puncture and foetotomy in a Malabari doe with concurrent live foetus delivered per vaginum is placed on record.
Acknowledgement
The authors are thankful to the Director, Animal Husbandry Department, Kerala, India and, the District Animal Husbandry Officer, Kannur, Kerala, India for providing necessary facilities for the study.
Conflict of Interests
The authors declare that there is no conflict of interests.
References



